General information
The sphincter of Oddi was first described back in 1681 by the British physician and anatomist Francis Gleason, but the sphincter received its name thanks to the Italian physiologist Ruggero Oddi, who published morphological observations on the structure of the sphincter in 1888, and also made the first manometry of the biliary tract.
Oddi is also the first to describe the dilation of the duct after removal of the gallbladder (cholecystectomy).
Located in the papilla of Vater (major duodenal) the sphincter of Oddi is a smooth muscle whose main function is to regulate the flow of pancreatic secretions and bile into the duodenum, and to prevent duodenal contents from entering the bile and pancreatic ducts.
Since the clinical picture of biliary tract dysfunction resembles other functional disorders of the digestive organs, the classification of these functional disorders has been revised several times.
Sphincter of Oddi dysfunction is identified as a separate functional disorder of the biliary tract according to the recommendation of the 1999 Rome Consensus (Rome II).
This clinical condition occurs more often in women 35-60 years old as a consequence of cholecystectomy, which was performed to eliminate calculous cholecystitis.
Sphincter of Oddi dysfunction is also observed in the presence of abnormal pancreatobiliary fusion and recurrent pancreatitis (the combination of sphincter of Oddi dysfunction with chronic pancreatitis is observed 4 times more often than chronic pancreatitis without a functional disorder of the sphincter).
How to treat sphincter of Oddi dysfunction
The basis of treatment for sphincter of Oddi dysfunction is:
- Diet therapy.
- Drug therapy necessary to relieve pain, as well as to eliminate symptoms of digestive disorders.
- Decontamination therapy. Used in the presence of bacterial overgrowth syndrome in the small intestine.
- Elimination of biliary insufficiency.
Anticholinergic drugs are prescribed to relieve muscle spasms. They prevent the neurotransmitter acetylcholine from interacting with the receptors of our body. Experts note their low effectiveness, and they also have a number of side effects. There are different types of anticholinergic drugs:
- metacin - prescribed for muscle spasm of internal organs;
- belladonna preparations - prescribed as an antispasmodic;
- platyphylline - also relaxes the smooth muscles of the gastrointestinal tract;
- buscopan - prescribed in connection with impaired motility of the gallbladder, biliary tract, cholecystitis, etc.;
- mebeverine (niaspam, duspatalin, sparex);
- hymecromon (odeston);
- papaverine;
- drotaverine;
- trimebutin (trimedat, neobutin);
- pinaveria bromide (dicetel).
Decontamination therapy involves the use of intestinal antiseptics (fluoroquinolones, enterofuril, etc.) and non-absorbable antibiotics (rifaximin).
In some types of pathology, papillosphincterotomy allows you to restore functionality: dissection of the large duodenal papilla. As an alternative, the doctor may prescribe endoscopic balloon dilatation (temporary catheters are installed), however, the effectiveness of this method has not been proven, and possible complications threaten pancreatitis.
As with any other ailments of the gastrointestinal tract, a successful outcome of treatment largely depends on adherence to diet. Diet therapy involves:
- exclusion of fatty foods;
- eating boiled and baked fruits and vegetables (since foods rich in fiber are especially useful for DSO);
- meals are frequent (5-6 times a day), in small portions.
The post How to treat sphincter of Oddi dysfunction appeared first on Administrator of the site Hangover.
You can contact the hepatologist in the comments. Don't hesitate to ask!
This article was last updated: 05/23/2020
Didn't find what you were looking for?
Try using search
doctor or administrator.
Read the dictionary of terms.
Expert author: gastroenterologist Daniela Sergeevna Purgina
Forms
The classification adopted according to the Rome II Consensus identifies the following types of sphincter of Oddi dysfunction:
- Biliary type I, which includes functional disorders accompanied by attacks of moderate or severe pain in the right hypochondrium or in the epigastric region. Repeated attacks last at least 20 minutes. ERCP reveals delayed removal of the contrast agent (the delay is more than 45 minutes). A double study of liver enzymes shows that the normal level of alkaline phosphatase or transaminases is at least 2 times higher than normal. The common bile duct is dilated by more than 12 mm.
- Biliary type II, in which the presence of typical pain attacks (biliary type) and compliance with at least one of the other criteria of type I are noted. Manometric examination confirms dysfunction of the sphincter of Oddi in 50–63% of cases. The identified disorders can be both structural and functional.
- Biliary type III, which is characterized by the presence of attacks of biliary pain in combination with the absence of objective disorders detected in patients of type I. A manometric study confirms the presence of sphincter of Oddi dysfunction only in 12–28% of cases (dysfunction is predominantly functional in nature).
- Pancreatic type, which is manifested by pain radiating to the back in the epigastric region (this type of pain occurs with pancreatitis). The pain decreases if you tilt your torso forward. Patients exhibit a significant increase in serum amylase and lipase. Manometry can detect sphincter of Oddi dysfunction in 39–90% of patients.
Reasons for development
Dysfunction of the sphincter of Oddi in patients occurs either as a result of sphincter stenosis, or due to primary functional dyskinesia (impaired contractions) of the sphincter.
The occurrence of anatomical stenosis of the sphincter of Oddi is provoked by inflammation and fibrosis, and in some cases, possible hyperplasia of the mucous membrane.
Inflammatory and fibrotic changes develop under the influence of small stones that pass through the common bile duct. There is also a hypothesis according to which inflammatory changes cause relapses of pancreatitis.
It is quite difficult to distinguish between functional stenosis of the sphincter of Oddi and an organic disorder, since these conditions can be caused by the same factor.
Dysfunction of the sphincter of Oddi is often detected in patients who have undergone gallbladder removal. In most cases, such patients experience insufficiency of the sphincter of Oddi, and as a result of this insufficiency, continuous flow of bile into the lumen of the duodenum occurs.
In addition, normally, under the influence of the neuropeptide hormone cholecystokinin, the gallbladder contracts, bile enters the duodenum and the sphincter of Oddi relaxes. Removal of the gallbladder can provoke hypertonicity of the sphincter of Oddi and dilation of the bile ducts. In some cases, after surgery, the tone of the sphincter of Oddi decreases, so insufficiently concentrated bile enters the intestine. In such a situation, infection of the bile is possible with the subsequent development of an inflammatory process in the bile ducts.
In some cases, there is no sphincter insufficiency, and attacks of pain are provoked by spasm (even moderate contraction of the sphincter when the gallbladder is removed causes a significant increase in pressure throughout the biliary tract, so the patient experiences pain).
Anatomical features
Where is the sphincter apparatus located? The valve is located on the inside of the duodenum - in the area of the papilla of Vater. The location of the sphincter of Oddi was described by F. Glisson almost 2 centuries ago. Research on this topic was published by R. Oddy in 1888.
The opening of the ducts occurs in 80% of cases simultaneously. When they are compressed, a so-called ampoule is formed. Digestive secretions accumulate in it.
The sphincter of Oddi controls the release of digestive juices into the duodenum. It prevents the backflow of small intestinal contents. The valve is responsible for filling the gallbladder and increasing pressure in the ducts to normalize the digestive process.
When digesting food, the sphincter of Oddi contracts rhythmically, which is necessary for the release of bile secretion. When not active, the valve is closed and its contractile function slows down. The secretion is not secreted, but accumulates in the area of the gallbladder.
Pathogenesis
Normally, in a healthy person, primary bile acids from the liver enter the bile ducts into the gallbladder, and from there they enter the duodenum during a reflex contraction of the gallbladder (occurs when stimulated by food). The formation of secondary bile acids occurs under the influence of anaerobic bacteria of the colon from primary bile acids.
Spasm of the sphincter of Oddi causes a violation of the passage (repeated entry) of bile into the intestines and is accompanied by various digestive disorders. As a result of irregular intake of bile acids, the following is observed:
- disruption of enterohepatic circulation of bile acids;
- impaired digestion and absorption of fats;
- a decrease in the bactericidal properties of duodenal contents, as a result of which the microbiocenosis of the small intestine is disrupted.
In case of insufficiency of the sphincter of Oddi, which occurs due to the inability of the sphincter to withstand increased pressure in the common bile duct in the absence of a gallbladder (performs a reservoir function), bile acids constantly enter the intestine. A constant supply of these acids can provoke the development of hologenic diarrhea. The damaging effects of bile acids on the mucous membrane of the stomach, esophagus and intestines largely depend on the conjugation of these acids and the pH of the environment, and these processes are influenced by the intestinal microflora.
Both with spasm and with insufficiency, as a result of changes in the composition of the intestinal microflora, the patient develops a dyspeptic symptom complex.
Factors predisposing to the development of dyskinesia include:
- hormonal changes (premenstrual period, pregnancy, taking hormonal contraceptives);
- stressful conditions;
- diabetes;
- diseases of the liver, pancreas and duodenum;
- operations affecting the stomach and bile ducts.
Causes and risk factors
Since dysfunction can be of both organic and inorganic nature, the reasons that cause it vary.
Impaired activity of the sphincter of Oddi of an organic nature (true stenosis) is a consequence of inflammation, hyperplasia or fibrosis of the duodenal mucosa.
Functional (inorganic) causes of the pathological condition include:
- diseases of the hepatobiliary zone;
- consequences of surgery (resection, gastrectomy) for stomach diseases;
- conditions after intestinal resection;
- endocrinopathies (hypo- and hyperfunction of the thyroid and parathyroid glands, diabetes mellitus, diseases of the adrenal glands);
- pregnancy;
- pharmacotherapy with hormonal drugs;
- metabolic diseases;
- systemic diseases (including autoimmune);
- conditions after cholecystectomy;
- taking medications that affect the tone and motor activity of smooth muscles;
- diseases of the stomach and pancreas (gastritis, pancreatitis, peptic ulcer of the stomach and duodenum).
Pharmacotherapy with hormonal drugs can lead to dysfunction of the sphincter of Oddi.
Risk factors for dysfunction of the sphincter of Oddi are:
- constant neuropsychic stress;
- excessive psycho-emotional stress;
- passion for unbalanced diets, including those based on strict restrictions on the amount of food taken.
Dysfunction of the sphincter of Oddi can have various origins. Treatment tactics will depend on the cause of pathological disorders. Only after the predisposing factor is eliminated can a lasting result from the measures taken be achieved.
Most often we are talking about violations of an inorganic nature:
- Diseases of the hepatobiliary system.
- Autoimmune disorders and hormone use.
- Metabolic disorders and systemic pathologies.
- Consequences of surgery.
- Pregnancy and thyroid diseases.
- Gastrointestinal diseases (gastritis, peptic ulcer, etc.).
Symptoms
Dysfunction of the sphincter of Oddi is accompanied by attacks of severe or moderate pain lasting more than 20 minutes, which are repeated for 3 or more months.
Also observed:
- feeling of heaviness in the upper abdominal cavity;
- painful, difficult digestion (dyspepsia);
- a feeling of dull, prolonged pain in the right hypochondrium.
The pain is rarely colicky in nature, but in combination with chronic pancreatitis, the pain can be very diverse - from biliary-type pain to pain reminiscent of an attack of biliary colic.
In most cases, painful attacks in patients at the initial stage of development of dysfunction occur quite rarely and last several hours, and between attacks the pain disappears completely. In some cases, the severity of pain and the frequency of attacks increases over time, and between attacks the pain does not disappear.
Painful attacks in most patients begin 2-3 hours after eating, but the connection with the nature of food and its intake is expressed differently in different patients (food can be fatty, spicy, etc.).
Increased pain can be caused by drugs that contain opium.
Since pain in young children is usually accompanied by a severe general reaction, dysfunction of the sphincter of Oddi in children is manifested by symptoms such as:
- fever (not lasting long);
- various vegetative reactions.
When children experience pain, they point to the navel area because they are not able to assess the location of the pain.
Diagnostics
Diagnostic criteria for sphincter of Oddi dysfunction include attacks of severe pain, which is localized in the epigastrium or right hypochondrium, if the pain:
- lasts more than 20 minutes;
- appears at least 1 time in the last year;
- the intensity interferes with normal activity, and the patient is forced to seek medical help;
- is not accompanied by structural changes that can explain the origin of pain.
Dysfunction of the sphincter of Oddi is suspected based on the results of laboratory tests performed during a painful attack or immediately after it (no later than 6 hours). Blood tests can determine the activity of pancreatic enzymes (amylase, lipase) and the level of liver enzymes (levels of aspartate aminotransferase, alkaline phosphatase and gamma-glutamyl transpeptidase), which increase 2 or more times during an attack. Since such indicators are also detected in other diseases, it is necessary to exclude choledocholithiasis and other disorders of the patency of the bile ducts.
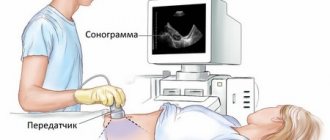
Non-invasive methods include:
- Ultrasound scanning with the introduction of provocative agents, which allows you to determine the diameter of the common bile duct and pancreatic duct. The diameter of the ducts is measured over an hour with an interval of 15 minutes (normally, the bile ducts do not change in diameter or the diameter decreases slightly). If the diameter increases by 2 mm or more, incomplete blockage of the biliary tract is suspected, but the cause of the blockage remains unclear.
- Cholescintigraphy, which helps determine dysfunction of the sphincter of Oddi in the presence of a delay in transit from the liver to the duodenum of the isotope with bile.
Invasive methods include:
- Endoscopic retrograde cholangiopancreatography (ERCP), which uses duodenoscopes with lateral optics. Thanks to this study, it is possible to determine the diameter of the ducts, exclude other diseases with similar symptoms and determine the time of emptying of the bile ducts.
- Endoscopic manometry of the sphincter of Oddi. It is considered the most reliable method, since it allows you to directly measure sphincter pressure using a triple-lumen catheter. A catheter connected to an external transducer is inserted through a duodenoscope (an instrument equipped with a video camera) into the common bile or pancreatic duct, and a recording device connected to the transducer records the data. Normally, the pressure in the common bile duct should be 10 mm Hg. exceed the pressure in the duodenum. With spastic contractions of the sphincter, the pressure rises to 110±25 mmHg. Endoscopic manometry also makes it possible to study individual indicators that reflect the motor activity of the sphincter (amplitude and frequency of phase contractions, frequency of retrograde contractions, etc.).
Since in 2–10% of cases, manometry contributes to the development of pancreatitis, the purpose of the study depends on the clinical picture and the patient’s response to conservative therapy.
Treatment
Drugs
Conservative measures to combat dysfunction of the sphincter apparatus:
- Nitrates (“Meatsin”). Aimed at blocking an attack.
- Antispasmodics (“Papaverine”, “No-shpa”). Helps cope with a painful attack.
- Calcium channel blockers (Nifedipine). Additional medications that are used to speed up recovery.
- Choleretic drugs (“Gimecromon”). Restores the production of digestive secretions.
Medications can cause side effects, so the dosage must be calculated individually. If you do not follow your doctor’s recommendations and take medications incorrectly, there is a high risk of worsening clinical symptoms.
If medications are ineffective, the doctor refers the patient to surgery. Recently, the operation has been replaced by the injection of botulinum toxin into the sphincter area.
To improve overall well-being and increase the effectiveness of medications, patients are advised to follow nutritional recommendations:
- The daily diet should be divided into 4-5 parts.
- It is necessary to exclude fatty, spicy foods.
- It is recommended to avoid fast food, fresh fruits and vegetables.
- Food must be subjected to gentle cooking.
To prevent bile stagnation, you need to adhere to recommendations such as a late dinner. Diet is a mandatory part of conservative therapy.
Digestion processes directly depend on the release of digestive juices into the intestinal lumen in the required volume. The sphincter of Oddi plays a leading role in regulating this process. It is a muscular ring that is located in the area of the bile and pancreatic ducts. Impaired sphincter motility can lead to the development of serious pathologies.
Not everyone knows the location of the sphincter of Oddi, formed by connective tissue elements and muscle fibers.
This structural element surrounds the end sections of the ducts of the gallbladder and pancreas, which allows you to regulate the release of digestive secretions, prevents the reflux of intestinal contents into the organs, increases the pressure in the duct, and accelerates the filling of the gallbladder.
Dysfunction of the sphincter of Oddi occurs when the tone of the organ increases, so the ducts expand, and unregulated secretion into the duodenum is noted. In this case, the concentration of bile may not reach normal values, which provokes infection and the development of symptoms of inflammation.
As a result, the following violations occur:
- Changes in the composition of intestinal microflora;
- Intestinal secretions lose their bactericidal activity;
- The process of breakdown and absorption of fats is disrupted;
- The normal circulation of fatty acids is altered.
Spasm of the sphincter of Oddi is an acquired disease, the main cause of which is muscular dyskinesia. The following factors provoke the pathological condition:
- Changes in the composition and rheological characteristics of bile;
- Passage violation;
- Intestinal dysbiosis;
- Surgical interventions;
- Structural changes in the sphincter that provoke the development of stenosis;
- Duodenitis.
Diseases of the gallbladder and sphincter of Oddi occur in patients at risk:
- Women during menopause, pregnancy, during treatment with hormonal drugs;
- Asthenic people;
- Development of emotional lability in young people;
- People whose work or life involves frequent stress;
- Patients after cholecystectomy (removal of the gallbladder);
- Patients with a history of diabetes mellitus;
- People with pathologies of the hepatobiliary system;
- Patients who underwent surgical treatment of the digestive organs.
Types of pathology
According to the modern classification, dysfunction of the sphincter of Oddi can take the following forms:
- Biliary type I. This usually includes disorders that provoke the occurrence of severe pain in the right hypochondrium. The duration of attacks does not exceed 20 minutes. ERCP reveals a decrease in the rate of removal of contrast, the following indicators increase: AST, alkaline phosphatase;
- Biliary type II. With this form of dysfunction of the sphincter of Oddi of the biliary type, characteristic painful sensations appear, 1-2 symptoms characteristic of type I pathology;
- Biliary type III. Only pain syndrome appears, there are no other symptoms.
- Pancreatic type. Spasm of the sphincter of Oddi causes pain in the epigastric region, which radiates to the back. Painful sensations decrease while bending the body forward. An increase in amylase or lipase is characteristic.
Clinical picture
Spasm of the sphincter of Oddi is characterized by the development of severe recurrent pain syndrome, which is localized in the area of the right hypochondrium, epigastrium. The pain usually radiates to the back or right shoulder blade. The duration of pain rarely exceeds 30 minutes. The pain syndrome can have varying intensity and often brings suffering to the patient.
Pain syndrome is often accompanied by the following symptoms:
- Nausea and vomiting;
- Bitter taste in the mouth;
- Belching air;
- There may be a slight increase in body temperature;
- The appearance of a feeling of heaviness.
- The listed symptoms usually worsen after eating fatty and spicy foods.
- Clinical symptoms of sphincter of Oddi dysfunction include:
- Increased liver enzymes;
- Slowing down the evacuation of contrast agent during ERCP;
- Expansion of the common bile duct.
Often dysfunction develops within 3-5 years after cholecystectomy. In this case, patients note an increase in pain, which is associated with the removal of the bile reservoir.
Important! The pain usually develops at night and cannot be relieved by taking painkillers or changing body position.
To determine the presence of sphincter dysfunction, doctors prescribe a laboratory blood test, which is performed during the development of pain or within 6 hours after it. This reveals elevated levels of amylase and lipase, aspartate aminotransferase, alkaline phosphatase and gamma-glutamyl transpeptidase.
Clinical symptoms may indicate the development of other diseases of the digestive tract caused by obstruction of the bile ducts. Therefore, the following instrumental diagnostic methods are widely used to confirm the diagnosis:
- Ultrasound. The scan is carried out while taking provocative agents, which makes it possible to assess the exchange of ducts. If normal values increase by 2 mm, incomplete blockage of the bile ducts can be suspected;
- Cholescintigraphy. The method allows you to determine sphincter motility disorders by the speed of movement of the injected isotope from the liver to the upper intestine;
- Endoscopic retrograde cholangiopancreatography (ERCP). The technique involves the introduction of duodenoscopes with lateral optics to assess the diameter of the ducts and determine the rate of their emptying;
- Manometry. The technique is based on the insertion of a triple-lumen catheter through a duodenoscope into the ducts to measure sphincter pressure.
Features of therapy
Treatment of sphincter of Oddi dysfunction involves relieving pain and other symptoms, normalizing organ motility and removing digestive secretions.
With the development of inflammation and dysbiosis, it will be necessary to eliminate the bacterial infection and normalize the intestinal biocenosis.
For this purpose, drug therapy, diet therapy, endoscopy and surgical treatment are widely used.
The following groups of drugs are widely used to eliminate dysfunction:
- Nitrates (Nitrosorbide, Nitroglycerin). The drugs help reduce the severity of pain;
- Anticholinergics (Biperiden, Akineton) help eliminate muscle spasm;
- Calcium channel blockers relax the sphincter of Oddi. Often cause adverse reactions, so they are rarely used;
- Antispasmodics (Papaverine, Pinaveria bromide, Drotaverine) eliminate spasms and pain;
- Myotropic antispasmodics. Mebeverine reduces sphincter tone and smooth muscle mobility. Gimecromone eliminates spasms and has a pronounced choleretic effect;
- To eliminate bacterial infection and dysbiosis, intestinal antibacterial drugs (Rifaximin, Enterofuril, fluoroquinolones), prebiotics and probiotics (Lactulose, Bifiform, Hilak forte) are used;
- Products based on ursodeoxycholic acid (Ursosan, Ursofalk) can eliminate biliary insufficiency.
Medical nutrition
Effective treatment of diseases of the digestive tract is impossible without following a special diet. If the sphincter of Oddi is malfunctioning, nutritionists recommend completely abstaining from fatty, spicy foods and fast food. The dishes consumed should be enriched with coarse fiber, which helps to normalize the motility of the digestive organs.
You should avoid eating fresh vegetables and fruits - the products must undergo heat treatment. Dishes should be boiled, stewed, baked, steamed. The daily diet should be divided into equal 6-7 servings, which are recommended to be taken every 3-3.5 hours.
Important! Having a late dinner just before bedtime helps avoid bile stagnation.
To increase the effectiveness of drug therapy, you can be treated with folk remedies. However, the use of traditional medicine recipes is possible only after consultation with a specialist. To normalize the functioning of the sphincter, the following medicinal raw materials are widely used:
- Corn silk. The plant is used to treat numerous pathologies of the hepatobiliary system. The raw material has pronounced choleretic and anti-inflammatory effects. To prepare the infusion, simply pour 20 g of corn silk into 200 ml of boiling water and leave the mixture for 1 hour. The product is taken 40 ml up to 5 times a day;
- St. John's wort herb. The raw materials are used to normalize the functioning of the liver and gall bladder, and to treat dyskinesia. To prepare a decoction, simply grind 1 tablespoon of the raw material and pour 250 ml of boiling water over the resulting mixture. The product is brought to a boil in a water bath and left for 1 hour. The decoction is taken 50 ml up to 3 times a day;
- Immortelle flowers. The plant is widely used to treat bile stagnation, hepatitis, and cirrhosis. To prepare the medicine, simply pour 2 tablespoons of crushed flowers into 250 ml of boiling water. The mixture is boiled for 10 minutes, cooled, and filtered. For the treatment of pathologies of the hepatobiliary system, it is recommended to take 50 ml of decoction 30 minutes before meals three times a day;
- Agrimony grass. Raw materials can alleviate acute and chronic hepatitis, cirrhosis, cholecystitis, and biliary dyskinesia. To prepare the infusion, simply pour 200 ml of boiling water into 1 tablespoon of crushed raw materials. The composition is infused for 2 hours, after which 100 ml are taken three times a day.
Therapy for this pathology is carried out on an outpatient basis, but sometimes, if the pain syndrome is severe, the patient may be hospitalized in the gastroenterology department to exclude catastrophes in the abdominal cavity and carry out diagnostics. The main directions of treatment for spasm of the sphincter of Oddi are relaxation of its muscles, pain relief, normalization of the outflow of bile and pancreatic juice. Diet therapy consists of eliminating fatty and spicy foods, spices, garlic and onions. It is important to normalize body weight, as well as quit smoking.
To eliminate spasm of the sphincter of Oddi, nitrates, anticholinergic drugs (metocinium iodide), and calcium channel blockers (nifedipine) are prescribed. Due to the fact that these drugs have side effects, as well as cardiovascular effects, it is advisable to use them in combination in small doses. Antispasmodics are also used (papaverine, pinaverium bromide, drotaverine); Mebeverine has sufficient selectivity for the sphincter of Oddi. In order to eliminate spasm, achieve a choleretic effect, and reduce biliary insufficiency, gimecromone is prescribed.
In the absence of proper results from conservative treatment, frequent relapses of pain and pancreatitis, surgical treatment is performed: endoscopic sphincterotomy, temporary balloon dilatation, temporary duct stenting. An alternative method is injection of botulinum toxin into the sphincter.
Forecast and prevention of spasm of the sphincter of Oddi
The prognosis for spasm of the sphincter of Oddi is favorable. In most cases, adequate long-term conservative therapy allows for sustainable clinical improvement; in its absence, sphincterotomy has a satisfactory effect. There is no specific prevention of spasm of the sphincter of Oddi. It is advisable to eat a balanced diet, maintain optimal body weight, and timely treatment of other diseases of the gastrointestinal tract.