Duodenal ulcers often begin gradually with sucking pain in the pit of the stomach, an increased feeling of hunger in the morning, and mild nausea.
But just as often, these signals that the body gives are not taken seriously. The person simply does not realize the scale of the impending problem. After all, persistent pain syndrome, as well as dangerous complications of this disease, develop much later.
If there is the slightest doubt about the presence of the disease, you should immediately contact a therapist or gastroenterologist with complaints, so as not to end up with a surgeon or, God forbid, a pathologist.
To help you navigate the variety of manifestations of duodenal ulcer, this article collects and highlights the main issues related to this disease.
What is an ulcer?
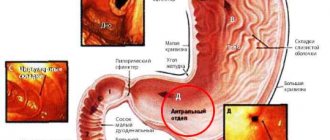
The wall of the duodenum, which is called duodenum in Latin, consists of mucous, submucosal and muscular layers. An ulcer is a wall defect, the bottom of which is located in the muscle layer, that is, the mucosa and submucosa are destroyed.
In the duodenum, the ulcer is most often located in the initial section (bulb or bulb), since here are the most favorable conditions for the reflux of acidic gastric contents and a wonderful place for the proliferation of bacteria that provoke peptic ulcer disease. Sometimes not one ulcer of the duodenal bulb is formed, but several at once. More often these are paired, opposite each other, “kissing” ulcers.
Peptic ulcer disease is the repeated formation of ulcerative defects in the wall of the duodenum, occurring with periods of exacerbation (the presence of an ulcer) and remission (the absence of an open defect in the intestinal wall). Since the ulcer heals with the formation of a scar, even in remission, scar defects remain on the mucous membrane. If exacerbations are frequent and a lot of scars are formed, they can deform or narrow the intestinal lumen.
About ten percent of the world's population suffers from duodenal ulcers. These are predominantly young and middle-aged people.
Stomach ulcer: causes
A defect in the mucous membrane is formed due to increased acidity of the gastrointestinal tract. Often, ulcerative lesions are caused by the activity of the microbe Helicobacter pylori. Bacteria can be present in a healthy body and not cause any consequences. However, a decrease in general immunity and active production of gastric juice sometimes leads to infection. The consequences of the activity of the bacterium can be not only a stomach ulcer, but damage to the duodenum, cancer, and gastritis.
Helicobacter pylori is the causative agent of gastrointestinal diseases
Aggressive factors influencing the development of pathology:
- Bad habits: smoking, alcohol abuse.
- Overwork, stress, lack of rest, lack of sleep.
- Unbalanced diet, non-compliance with the regime, junk food.
- Long-term use of potent medications.
- Vitamin deficiency, strict diets.
- Abdominal injuries, burns.
- Chronic diseases.
PUD is not a hereditary pathology. But an infection caused by the Helicobacter microorganism can be transmitted to family members through close contact. Most often, a stomach ulcer is formed against the background of several problems: overexertion, unsystematic nutrition, weakened immunity.
Why does she appear?
There is no single view on the occurrence and development of duodenal ulcers. There are several equivalent theories of the occurrence of ulcers.
- On the one hand, several years ago there was a very popular assumption that peptic ulcer disease is the result of the colonization of the stomach and intestines by a microbe such as Helicobacter pylori. The microbe infects cells that secrete mucus. During development, it quickly colonizes the stomach and duodenum, stimulating the release of gastrin and releasing cytokines (substances that damage cells). Later it turned out that not all types of this microorganism living in humans cause disease. Therefore, blaming everything on infection is still wrong.
- An earlier assumption was an imbalance between the ability of the mucous membrane to defend itself and aggressive factors in the form of gastric acid and pepsin, which enter the intestine when the function of the obturator muscle of the gastric outlet is insufficient. It was also believed that the intestine was scratched by rough food. Today, these assumptions have been supplemented by the fact that a decrease in protective prostaglandins has been found in the mucous membrane of patients with peptic ulcer disease.
- A relationship has been found between the incidence of ulcers and blood type. Carriers of the first group with a Rh-positive factor are at greater risk.
- Soviet physiology was of the opinion that ulcers develop in people with excessive irritation of the cerebral cortex against the background of chronic stress or nervous experiences, when the release of gastric juice and inflammatory mediators (gastrin) is stimulated through the autonomic nervous system.
- Another interesting conclusion is associated with gastrin: prolonged exposure to the sun stimulates the release of this hormone and, accordingly, provokes an exacerbation of peptic ulcer disease or worsens its course.
- Taking medications such as corticosteroids and non-steroidal anti-inflammatory drugs can provoke ulcerations of the intestinal mucosa.
- Alcohol and nicotine worsen the condition of the mucous membrane, change the nature of the secretion of hydrochloric acid and pepsin by the stomach, affect the level of gastrin and somatostatin, and also reduce the protective properties of the mucus. Alcohol directly damages mucosal cells.
What are the symptoms of a duodenal ulcer?
The symptoms of stomach and duodenal ulcers are very close to each other. These are: pain, heartburn, nausea, vomiting, appetite disorders.
- Pain
With ulcers, the duodenum is called late. They occur an hour and a half after eating. Hunger pains that occur if food has not been received for more than 4 hours are also characteristic. A type of such pain is night or early morning, similar to very acute hunger and sucking in the right hypochondrium. The nature of pain may vary from patient to patient. There are stabbing, aching, cutting, sucking or spasmodic pains of varying intensity and duration. In this case, the pain is located in the right half of the epigastric region (bulb ulcer). They can radiate to the right hypochondrium or to the back. With an ulcer located at the end of the intestine, the pain shifts more to the midline of the epigastrium or to its left half. The basis of the pain is a violation of the integrity of the intestinal wall, inflammation and accumulation of under-oxidized metabolic products.
- Heartburn
accompanies about a third of duodenal ulcers. It is due to the fact that the acidic contents of the stomach are thrown into the esophagus against the background of impaired motor activity of the stomach and intestines and inflammatory changes in the mucous membrane.
- Nausea and vomiting
eaten food or gastric contents are characteristic of high duodenal ulcers. With the development of secondary inflammation of the pancreas or gallbladder against the background of a peptic ulcer, vomiting of bile may occur.
- Appetite disorders
can manifest itself as an increase (sucking in the stomach is somewhat smoothed out by food intake) or an aversion to food and fear of it, since in the presence of an ulcer, food can provoke pain.
Complications of the disease
Peptic ulcer
With stomach and duodenal ulcers, serious complications are possible:
- Perforation (formation of a through wound) and loss of food into the abdominal space threatens the development of peritonitis; digestive juices destroy body tissue, which can cause damage to large vessels, bleeding and death . Symptoms are increased body temperature, release of sticky sweat, vomiting, decreased blood pressure, and limbs become cold.
- Penetration. The integrity of the wall is also compromised, but the contents enter the small intestine, pancreas, and liver. The pain becomes unbearable and constant, radiating to the right shoulder or back. Threatens organ damage and death. Painkillers do not help and urgent surgery is required.
- Pyloric stenosis is an anatomical change in the sphincter (narrowing) connecting the stomach and duodenum. When a scar forms, food cannot travel further down the digestive canal. When food stagnates metabolic processes are disrupted , an unpleasant odor appears when breathing, vomiting and a full stomach often occur.
- Bleeding. Duodenal ulcers are characterized by bloody stools, while gastric ulcers are characterized by bloody vomiting. This is a very dangerous condition, because with massive hemorrhage it can lead to death within 20 to 40 minutes. Requires urgent hospitalization.
- Cancerous degeneration of an ulcer – malignancy. Most common for stomach ulcers. Cancers of the duodenum are rare. Stomach cancer is more common in older people. Characteristic changes in taste, constant pain, the person loses weight.
It is better to constantly monitor nutrition and immunity than to treat gastric and duodenal ulcers in an advanced stage, because digestive disorders interfere with recovery and the process drags on for many months. Prevention of stomach and duodenal ulcers consists of following basic nutritional rules , a balance of proteins, fats and carbohydrates. A positive psychological attitude is of great importance, making it easier to tune in and believe in recovery.
What does an ulcer look like?
Important! Complications of gastric and duodenal ulcers in some cases occur suddenly, without obvious symptoms, so if you have stomach problems, you need to monitor your well-being and call doctors in time to provide assistance.
Complications of peptic ulcer
If the ulcer is not detected and treated in a timely manner, it may heal on its own. However, there is a high risk of developing a number of complications, which not only aggravate the course of the disease, but complicate treatment and worsen the prognosis for the patient. All complications are divided into:
Destructive - destroying the intestines:
- it's bleeding
- perforation - perforation
- penetration - penetration into a neighboring organ
Dysmorphic complications that change its structure:
- malignancy - the development of a malignant tumor at the site of the ulcer
- cicatricial deformation - a change in the structure of the walls and narrowing of the intestinal lumen until it is completely closed due to scars from ulcers.
Ulcers located on the anterior wall of the intestine are more likely to perforate. Ulcers of the posterior wall often penetrate the head of the pancreas.
Ulcers or erosions?
Many people confuse ulcers on the walls of the stomach with erosions on its mucous membrane. However, this is wrong. Erosive defects most often affect only the mucous membrane of the organ, while ulcerated areas are characterized by deeper lesions. That is, the damage penetrates both the submucosal and muscular tissues of the stomach.
It is clear that ulcers manifest themselves in more severe pain than, for example, erosion or ordinary inflammation. In addition, they are more difficult to treat and heal more slowly. After the ulcers heal, deep scars form that may not disappear for decades.
Why does such an unpleasant and painful disease occur? Let's find out.
Bleeding from the duodenum
Physical work and heavy lifting can provoke bleeding. But most often the cause is alcohol intake, if treatment with medications is not carried out or is inadequate. Therefore, up to 80% of this complication occurs in men. In this case, blood loss can be of different volumes.
When bleeding occurs, tar-colored stools or vomit with a color similar to coffee grounds appear. Minor bleeding may only result in diarrhea or pasty, dark stools. At the same time, with heavy blood loss, vomiting will be accompanied by rapidly increasing weakness, dizziness and even loss of consciousness. Bleeding is an emergency that requires calling an ambulance or going to a hospital emergency room on your own.
Symptoms of a perforated duodenal ulcer
Perforation of an ulcer means not only bleeding, but also the entry into the abdominal cavity of the contents of the duodenum, where pancreatic enzymes and bile are released. These are quite aggressive substances that quickly cause irritation of the peritoneum and lead to inflammation of the abdominal cavity (peritonitis).
If acute stabbing pain in the abdomen occurs against the background of a peptic ulcer, you should immediately call an ambulance. This pain appears more often in the right half of the epigastric region and can radiate to the right shoulder or scapula. The pain is so severe that the patient takes a forced position, lying on his side or back with his legs brought to his stomach. At the same time, the skin becomes very pale. The abdominal muscles tense, the person avoids any movement.
The most dangerous period is the period of imaginary well-being, which develops a few hours after the onset of perforation. Here the pain subsides somewhat, the patient begins to move and assures that he is feeling better. During this period, patients often recklessly refuse surgery that could save their life. But, if 6-12 hours pass from the onset of perforation, and the patient does not undergo surgery, his condition will sharply worsen:
- vomiting appears
- temperature increase
- the pain will return
- bloating will appear
- pulse and heartbeat increase
- peritonitis will develop, which will need to be operated on, and the prognosis for which at this stage is already worse.
Signs and symptoms of stomach ulcers
Knowing the main symptoms of a developing pathological process will allow you to quickly consult a doctor for help and diagnose the disease, which guarantees the success of therapeutic intervention without surgical intervention. However, sometimes a stomach ulcer does not manifest itself at all, which indicates the need for regular examination. As a rule, an asymptomatic course of the ulcerative process is observed in 25–28% of cases, and the presence of an ulcer is detected after the death of the patient.
You can suspect a gastric ulcer based on the following signs:
- Pain sensations localized in the upper abdomen. This symptom occurs in 75% of cases. Half of the patients complain of feelings of low intensity, in the remaining 50% they are more pronounced and intensify during physical activity, after ingesting alcohol or spicy food, during long breaks between meals;
- Heartburn. It is expressed in a burning sensation in the epigastric region. It occurs due to the fact that the acidic contents of the stomach, which has an aggressive environment, enters the lumen of the esophagus, irritating its walls. This symptom is observed frequently and occurs in 80% of patients. Heartburn usually appears 1-2 hours after eating;
- Feeling of nausea, sometimes accompanied by vomiting. This symptom occurs due to impaired gastric motility. With an ulcer, vomiting occurs 1.5-2 hours after eating and, as the stomach is emptied, brings a feeling of relief. Therefore, patients often induce vomiting on their own;
- Decreased appetite during peptic ulcer disease may be associated with a person’s fear of experiencing pain or with gastrointestinal motility disorders;
- Belching, which is characterized by the uncontrolled reflux of gastric juice into the oral cavity. In this case, the patient feels bitterness or a sour taste in the mouth;
- Increased gas formation;
- The appearance of a feeling of heaviness in the abdominal area, observed after eating;
- Quickly coming feeling of satiety;
- Stool disorders. Most often, patients complain of constipation, and diarrhea is not typical for peptic ulcer disease. Up to 50% of patients experience difficulties with bowel movements, especially during exacerbation of a stomach ulcer.
Among the external signs of a stomach ulcer, it is especially worth noting the presence of a gray coating on the tongue, which almost always indicates problems with the gastrointestinal tract. The patient may suffer from increased sweating of the palms and experience pain when pressing on the epigastric region.
Pain due to stomach ulcer
The nature of the pain largely depends on where the lesion is located.
Depending on the complaints made by patients, the doctor is able to suspect an ulcer of one or another part of the stomach:
- When the subcardial and cardiac sections are affected, the feeling of pain begins to bother you early, about 20 minutes after eating. In this case, unpleasant sensations are localized quite high - at the very xiphoid process of the epigastric region. Often such pain can radiate to the heart and be incorrectly differentiated. Their clear relationship with food intake can be traced, but there are no parallels with physical activity. Relief comes from drinking milk or antacids. As for intensity, the pain is mild. They are often accompanied by vomiting, belching, and heartburn.
- When the lesser curvature of the stomach is affected, pain occurs in the epigastric region, which is located to the left of the midline of the abdomen. Their start time after eating is on average 1 hour. After the stomach copes with its task, the pain goes away. Patients often complain of discomfort after long breaks in food, as well as in the evening and night hours. The intensity of the pain is moderate, the nature is aching. When the process worsens, the pain becomes very pronounced. The patient often feels nauseous, but rarely vomits;
- When the greater curvature of the stomach is affected, the pain is of low intensity, which makes it difficult to diagnose this type of ulcerative lesion. Moreover, it is precisely this ulcer that is often malignant in nature, although it is rare;
- When the antrum is affected, pain often occurs in the evening and at night, accompanied by sour belching and heartburn. Localization – epigastric region;
- When the pyloric canal is damaged, the pain is quite intense, and its character is paroxysmal. One attack can last up to 40 minutes. There are pains at night and when hungry, but in some patients there is no connection between food intake and pain. Saliva production increases, and persistent and prolonged heartburn often occurs.
Sometimes doctors encounter atypical manifestations of the ulcerative process. In this case, pain may occur in the right hypochondrium, in the right iliac region, in the lumbar region, in the heart region, or not appear at all. All this makes diagnosing the disease difficult and often leads to complications.
Cicatricial stenosis of the duodenum
If exacerbations of duodenal ulcer follow one after another or the ulcerative defects are very large and deep, scars from ulcers can significantly deform or narrow the intestinal lumen. In this case, problems arise with the passage of food, and a narrowing (stenosis) of the intestine develops, which requires surgical treatment. Clinically, decompensated stenosis is manifested by vomiting, impaired passage of food and distension of the stomach. At the same time, disturbances in the content of salts and water in the body develop, which lead to lethargy, weakness, drowsiness, increased muscle tone, and a feeling of goosebumps running on the skin of the arms and legs.
Diagnostics
Today, the main and most informative method for identifying peptic ulcers is FGDS (fibrogastrodudenoscopy), in which, by inserting an endoscope (optical probe) into the stomach and duodenum, you can see the ulcer, assess its size and depth, and take the mucous membrane for examination (biopsy). or conduct a rapid urease test for the presence of Helicobacter pylori.
X-ray diagnostics, which is indispensable in clarifying complications, is of auxiliary importance.
Patients are also prescribed a clinical blood test, blood biochemistry, and a stool test for the Gregersen reaction (detection of occult blood).
Diagnosis of stomach ulcers
The reason for referring the patient for diagnostics to establish a gastric ulcer is complaints of pain associated with the process of eating. You should not hesitate if the pain is accompanied by vomiting or nausea.
Diagnostics consists of several stages:
- First, the patient will need to donate blood, urine and feces for a general analysis, as well as donate feces for occult blood. If a general blood test shows the presence of anemia, a decrease in the number of red blood cells against the background of an increase in ESR, then this indicates the presence of an inflammatory process;
- FEGDS, when the doctor, using a special tube with a camera at the end, thoroughly examines the gastric mucosa. At the same time, it is possible to take material for a biopsy;
- Ultrasound of the gastrointestinal tract (stomach, gallbladder, liver and pancreas);
- Carrying out x-rays of the affected organ using a contrast agent. Although this method is now considered obsolete;
- Monitoring the pH of gastric juice during the day and pH-metry. This is a rather painful method, as it is invasive. It allows you to assess the aggressiveness of gastric juice in relation to the mucous membrane lining it.
It is advisable that special tests be carried out to determine the presence of the Helicobacter pylori bacterium in the human body.
To do this you need:
- Detection of antibodies to them in the blood (serological method);
- Carrying out a stool test (detection of antibodies to Helicobacter pylori in the patient’s stool);
- Breathing radionuclide urease test (the urea exhaled by a person, which is secreted by bacteria, is determined);
- Rapid urease test (testing of the gastric mucosa after FEGDS).
If there are indications, the patient is sent for an X-ray examination of the stomach, CT scan, endoscopic ultrasonography, etc.
The main thing is to exclude the presence of complications, in particular bleeding, as soon as possible.
Treatment of duodenal ulcers
With timely detection of duodenal ulcer in the acute stage, treatment is reduced to the prescription of conservative therapy (prescription of tablets, less often injections or drips). The times when surgical treatment methods were used for uncomplicated peptic ulcers are a thing of the past. If the peptic ulcer is complicated, then hospitalization in a surgical hospital is mandatory, and refusal to do so can be fatal. This does not mean that any bleeding will be operated on, but timely observation is indicated for every complicated duodenal ulcer.
Previously, it was customary to carry out seasonal (spring and autumn) preventive treatment of duodenal ulcer. Currently, this practice is not supported, as it has not brought the expected results. Treatment is prescribed for the period of exacerbation of duodenal ulcer.
Clinical picture of peptic ulcer
The most consistent and important symptom of peptic ulcer disease is pain. Pain in peptic ulcer disease has a clearly defined rhythm (time of occurrence and connection with food intake), and seasonality of exacerbations.
Based on the time of occurrence and their connection with food intake, pain is distinguished between early and late, night and “hungry”. Early pain occurs 0.5–1 hour after eating, lasts 1.5–2 hours and decreases as gastric contents are evacuated. Such pain is more typical for gastric ulcer in the upper part.
Late pain appears 1.5–2 hours after eating, night pain occurs at night, and “hungry pain” occurs several hours after eating and stops after eating. Late, night and “hungry” pains are more typical for the localization of an ulcer in the antrum of the stomach or duodenal ulcer.
The nature and intensity of pain may vary (dull, aching, burning, cutting, cramping). The localization of pain in peptic ulcer disease is different and depends on the location of the ulcer: with an ulcer on the lesser curvature of the stomach, pain often occurs in the epigastric region, with duodenal ulcers - in the epigastric region to the right of the midline. With ulcers of the cardial part of the stomach, pain can be behind the sternum or in the heart area; in this case, it is important to differentiate peptic ulcer disease from angina pectoris or myocardial infarction. Pain often occurs after taking antacids, milk, food, and even after vomiting.
In addition to pain, the typical clinical picture of peptic ulcer disease includes various dyspeptic symptoms.
Heartburn is one of the early and frequent symptoms characteristic of peptic ulcer disease. Heartburn can occur at the same time after eating as pain. It often precedes the onset of pain, and subsequently is often combined with pain. These two symptoms are closely related, and some patients have difficulty distinguishing between them. In later stages of the disease, heartburn may disappear. But sometimes it can be the only subjective manifestation of a peptic ulcer.
Belching is a fairly common, but not specific symptom of peptic ulcer disease. The most typical belching is sour. The appearance of belching is associated with impaired evacuation of gastric contents due to prolonged spasm and severe inflammatory edema of the pylorus or duodenal bulb. It should also be remembered that belching is characteristic of a diaphragmatic hernia.
Nausea and vomiting are dyspeptic symptoms characteristic of exacerbation of peptic ulcer disease. Nausea is often accompanied by vomiting, although vomiting can occur without preceding nausea.
Vomiting in patients with peptic ulcer disease often has some specific features: firstly, it occurs at the height of pain, being, as it were, the culmination of pain; secondly, it brings significant relief. Vomit, as a rule, has an acidic reaction with an admixture of recently eaten food. Vomiting can also occur on an empty stomach.
Appetite in case of peptic ulcer is usually preserved or even increased (the so-called painful feeling of hunger). Decreased appetite is possible with severe pain syndrome; fear of eating may occur due to the possibility of pain occurring or increasing. Decreased appetite and fear of food can lead to significant weight loss for the patient.
Constipation is observed in half of patients with peptic ulcer disease, especially during exacerbation. Constipation in peptic ulcer disease is caused by a number of reasons: spastic contraction of the colon, a gentle diet, poor coarse fiber and the resulting lack of intestinal stimulation, limitation of physical activity, and the use of antacids (Almagel, etc.).
Symptoms depend on the location of the ulcer and the age of the patient . In some cases there may be no pain (painless ulcers). In these cases, ulcers are discovered when complications develop (ulcer bleeding, ulcer perforation - breakthrough of the ulcer wall into the abdominal cavity, penetration of the ulcer). Only about half of people with duodenal ulcers (duodenal ulcers) have typical symptoms. In children, the elderly, and patients taking certain medications, symptoms may be atypical or absent altogether.
Diet for ulcers
In case of duodenal ulcer, a 4g diet is prescribed for the period of exacerbation, which involves mechanical, chemical and temperature sparing. It is recommended to eat 5-6 meals a day in small portions. Food should be heated to a temperature of 36-37 degrees. Hot, cold and dry foods are excluded (see what you can eat with gastritis). Alcohol and smoking on an empty stomach are prohibited.
- Preference is given to boiled, pureed food. Slimy porridges, non-rich creamy soups, mashed potatoes, pasta, rice and buckwheat are desirable. Steamed fish, poultry, boiled meat in the form of soufflé or minced meat and cutlets. Watermelons and bananas are allowed as fruits.
- You will have to give up fried, spicy, rich meat and bone broths, marinades, soda, strong tea, coffee, and yeast baked goods. The greatest harm is caused by fruits and vegetables containing fiber. You will have to forget about tomatoes, cucumbers, apples, pears, cabbage, carrots, radishes and other garden delights until the ulcerative defect heals.
- It is strictly forbidden to chew gum, which stimulates gastric secretion.
- Milk in this situation becomes an ambiguous product. In some patients, whole milk can irritate the ulcer due to calcium ions, while others drink it with pleasure, as it significantly reduces heartburn.
For more details, see Diet for duodenal ulcers, list of products, menu.
Diet
Special requirements are put forward for food. It should spare the mucous membrane from mechanical and chemical damage and at the same time be complete. Meals should be fractional 5-6 times a day. All dishes must be chopped or consumed in liquid form, steamed or boiled, neither cold nor hot.
What foods can you eat if you have a stomach ulcer, and what can you not: list
| Foods you can eat | Products to exclude |
|
|
Drug treatment of duodenal ulcers
Peptic ulcer of the duodenum is currently treated with the following groups of drugs.
Medicines that reduce the production of gastric juice
The leading positions in this group are held by proton pump blockers, which slow down the secretion of hydrochloric acid:
- Products based on omeprazole - omez, gastrozole, bioprazole, demeprazole, lomac, zerocid, krismel, zolser, omegast, losek, omezol, omitox, omepar, zhelkizol, pepticum, omipix, promez, pepticum, ricek, orthanol, romsec, sopral, ultop , chelicide, cisagast, chelol.
- Medicines based on pantoprazole - controloc, sanpraz, nolpaza, peptazole.
- Lansoprazole preparations - helicol, lanzap, lansofed, lanzotope, epicure, lancid.
- Based on rabeprazole - zulbex, zolispan, pariet, ontime, hairabezol, rabeloc.
- Esomeprazole - Nexium.
H2-histamine receptor blockers have practically ceased to be used to treat peptic ulcers, as they cause withdrawal syndrome (with abrupt cessation of use, the symptoms of the disease return).
- These are ranitidine (Gistac, Rannisan), famotidine (quamatel, ulfamid, gastrsidine), cimetidine (Belomet).
Selective blockers of M-cholinergic receptors (gastrocepin, pirencipin) reduce the production of pepsin and hydrochloric acid. Used as auxiliary medications for severe pain. May cause palpitations and dry mouth.
Agents that increase the protective properties of the mucous membrane
- Sucralfate (Venter) forms a protective coating at the bottom of the ulcer.
- Sodium carbenoxolone (Ventroxol, Biogastron, Kaved-s) accelerates the restoration of the epithelium of the mucous membrane.
- Colloidal bismuth subcitrate (de-nol) forms a film on the ulcer.
- Synthetic prostaglandins (enprostil) stimulate mucus production and cell restoration.
Other drugs
- Medicines that calm the central nervous system. Tranquilizers (seduxen, elenium, tazepam), antidepressants (amitriptyline), sedatives (tenoten, valerian preparations, see sedatives).
- Blockers of central dopamine receptors (metoclopramide, raglan, cerucal) normalize intestinal motor activity.
The course of treatment for ulcers can take from two to six weeks, depending on the size of the defect and the general condition of the body.
It should be noted that a competent doctor who can monitor the treatment process and evaluate its results should prescribe treatment for duodenal ulcers, select medications and dosage regimens.
Treatment of duodenal ulcers with antibiotics
Antibiotic therapy for peptic ulcers has appeared since the undoubted participation of Helicobacter pylori microorganisms in the development of the disease was proven. In the early stages of the use of antibiotics, it was believed that the war should be waged until a victorious end, that is, the complete disappearance of the microbe, which was confirmed by culture, a urease test during FGDS, or a blood test for antibodies to the bacterium. Later it turned out that not all types of Helicobacter cause disease, that it is unrealistic to destroy all Helicobacter, since when it dies in the stomach and duodenum, it moves to the lower intestines, causing severe dysbiosis and inflammation.
Re-infection is also possible when using someone else's or shared utensils and the same FGDS, which therefore must be performed only according to strict indications.
However, today it is advisable to carry out one or two courses of therapy with antibacterial drugs (amoxicillin, clarithromycin or tetracycline) for proven Helicobacter infection. If after one course of antibiotics the bacteria are not killed, then this drug is not worth repeating. A different treatment regimen is selected.
Causes of stomach or duodenal ulcers
Peptic ulcer of the stomach and duodenum can be caused by both external and internal factors.
External causes of stomach and duodenal ulcers
Presence of Helicobacter pylori. It is transmitted by contact through food and water, saliva and dirty dishes, during various manipulations in case of poor sterilization of instruments (ENT, gastroenterology) and from mother to fetus.
Violation of diet and eating habits - eating large amounts of fatty, hot or spicy foods.
Smoking and alcohol abuse.
Long-term use of corticosteroids, non-steroidal anti-inflammatory drugs (salicylates, Diclofenac, Ibuprofen), cytostatics (Imuran, Fluorouracil), Reserpine.
“Stress ulcers” – resulting from burns, frostbite, trauma and all types of shock.
Domestic
- Hereditary predisposition.
- Lack of enzymes and vitamins.
- Hyperparathyroidism.
- Diabetes.
- Reflex effects in the presence of diseases of the abdominal organs - pancreatitis, cholecystitis, appendicitis, hyperacid gastritis.
- Chronic infections - tuberculosis, syphilis, chronic bronchitis.
- Kidney and liver failure.
- Sarcoidosis.
- Disorder of the blood supply due to vascular spasm, leading to ischemia of the gastric or duodenal mucosa.
- Acute or chronic stress.
Faringosept, instructions for use
Ulcer treatment regimen
First line Helicobacter pylori eradication scheme:
- Double dose proton pump inhibitor twice daily (eg 40 mg omeprazole or esomeprazole twice).
- Clarithromycin 500 mg twice daily or Josamycin 1000 mg twice daily.
- Amoxicillin 1000 mg 2 times a day.
- De-nol 240 mg twice a day.
Scheme of the second row (in the absence of FGD dynamics of ulcer size)
- Proton pump inhibitor in double dose 2 times a day (same as scheme 1)
- De-nol 240 mg twice a day.
- Metronidazole 500 mg three times a day.
- Tetracycline 500 mg 4 times a day.
Before starting therapy, Helicobacter pylori is detected using an immunological blood test (antibodies to the pathogen). Control – detection of Helicobacter antigens in feces. The urease breath test is not very informative.
The duration of eradication therapy is from 10 to 14 days. If treatment is ineffective with sequential regimens 1 and 2, Helicobacter pylori is typed and its sensitivity to drugs is determined.
Today, regimens with levofloxacin can only be used in regions of the Russian Federation where Helicobacter remains sensitive to this drug.
If duodenal ulcer is not associated with Helicobacter pylori infection, then treatment is carried out with medications that reduce the production of gastric juice. After 7-14 days of combination therapy, treatment is prescribed for another five weeks.
Alternative treatment for duodenal ulcers
Complete or partial distrust of traditional medicine most likely does not bode well for an ulcer sufferer. There are drugs for the treatment of ulcers, the effect of which has been proven in serious random studies in humans. Also, the effect of drugs is checked by everyday medical practice. Schemes are being refined and side effects of drugs are being identified. At the same time, no one canceled the alternative possibility of being treated with folk remedies.
Freshly squeezed potato juice is considered one of the most effective traditional medicine for stomach and duodenal ulcers. It tastes rather unpleasant, but you can get used to it quite easily. It is better to use the Morning Rose or American varieties, but any unspoiled potato tuber will do. Preparing juice is quite labor-intensive, given that you only need to drink it fresh and 3 times a day, but you can get the hang of it if you want. The raw potato tuber is peeled, grated and squeezed through several layers of gauze. The juice should be drunk immediately, otherwise it turns black and loses its medicinal properties. The first 3 days only take a tablespoon before meals 30 minutes, preferably 3 times a day, then 3 days 2 tablespoons, gradually increasing to half a glass per dose and so on for 21-28 days. This requires adherence to a diet. After 2-3 weeks the course can be repeated. This really helps!
You can resort to traditional medicine, use treatment with sea buckthorn or olive oil (1 dessert spoon on an empty stomach for 3 months), honey, propolis, herbs (calendula, plantain, St. John's wort), after going on a duodenum-friendly diet and taking twice a day 20 mg omeprazole daily.
Author:
Postnova Maria Borisovna general practitioner