Home / Endocrinologist / Treatment of hormonally active tumors of the pancreas
Hormone-active pancreatic tumors belong to the apudom group. They are more often benign.
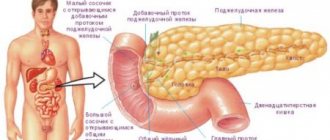
Pancreatic tumors
– neoplasms with varying degrees of cellular differentiation, emanating from the tissues of the endocrine or exocrine part of the pancreas.
Benign neoplasms often do not appear until they reach a large size; malignant - characterized by tumor intoxication, compression syndrome of surrounding vessels, nerves, and organs.
Symptoms of hormonally active pancreatic tumors
Depending on the hormone released into the blood by tumor or (less often) hyperplastic cells scattered in the tissues of the organ, certain clinical manifestations of the disease are observed.
Three types of tumors have been studied better than others:
- g lucagonoma,
- insulinoma (insuloma),
- gastrinoma.
Symptoms of hormonally active pancreatic glucagonoma:
Glucagonoma is a tumor of the a-cells of the pancreas. It manifests itself as gynerglucagonemia (glucagon is an insulin antagonist) and diabetes mellitus. Due to the catabolic properties of glucagon, the following develops:
- cachexia,
- anemia
- and peculiar necrotic changes in the tissues of the oral cavity and on the skin, simulating pellagra.
Symptoms of hormonally active insulinoma:
Insuloma (insulinoma) comes from the β-cells of the islets of Langerhans and manifests itself as hyperinsulinism - recurrent hypoglycemia, leading to seizures and organic changes in the brain.
Manifestations of hormonally active gastrinoma of the pancreas
A peculiar syndrome has been described, which was characterized by gastroduodenal ulcerations resistant to routine therapy. They occurred with pronounced clinical manifestations, excitable gastric hypersecretion, and often with severe complications.
Types of tumors
Pancreatic tumors are classified into benign and malignant tumors. An accurate diagnosis is based on the location, changes in cellular structures (histology), and the effect on the normal functionality of the organ.
Currently reading: Characteristics and treatment methods for pancreatic necrosis
The tumor can develop in the body, tail, and head of the organ. Malignant cells can have the following types:
- Adenoma;
- Acinar cell carcinoma;
- Adenocarcinoma;
- Squamous cell carcinoma.
Cells formed as a result of endocrine disorders have names such as gastrinoma, insulinoma, carcinoid.
A type of malignant tumor is blastoma, which occurs during intrauterine development, which contributes to the formation of cancer in childhood.
The stage of the oncological process depends on the size of the resulting formation:
- The formation of mutated cells, which are characterized as “cancer in the zero stage”;
- The first stage implies the presence of a tumor measuring 2 cm without pronounced clinical symptoms;
- At the second stage, the growth of cancer cells and the spread of metastases are noted;
- The third stage involves damage to the portal vein and other large organs;
- At the fourth stage, the patient’s general condition is unstable, and examination reveals extensive metastases throughout the body.
Benign tumors develop slowly and do not metastasize, since the cells do not change differentiation. When performing an ultrasound, a formation with hypoechoic edges containing fluid inside is clearly visualized.
Diagnosis of hormonally active pancreatic tumors
Timely diagnosis and accurate determination of the type of pancreatic tumor requires coordinated work
- gastroenterologist,
- surgeon
- endoscopist.
Without the use of modern methods of visualization and chemical typing of tumors, it is almost impossible to identify a pancreatic tumor.
It should be remembered that even the most modern diagnostic devices and techniques are not always able to answer the question about the nature of organ damage; the clinical experience of the attending physician is of great importance when diagnosing neoplasms of the pancreatic zone.
Damage to the pancreas will be indicated by studies such as
- blood chemistry,
- coprogram
- study of the secretion of digestive juices during esophagogastroduodenoscopy.
- gastrography and duodenography,
- magnetic resonance cholangiopancreatography,
- magnetic resonance imaging of the pancreas,
- computed tomography of the biliary tract.
After identifying a tumor in the tissues of the pancreas (the size of the tumor can vary from 2 mm to 200 mm), the level of hormones and metabolites in the blood is determined (adrenaline, norepinephrine, serotonin, cortisol, gastrin, vasoactive peptide, insulin, glucagon, pancreatic and C-peptide , somatostatin, etc.) and tumor markers (CA19-9, CA 50, CA 242, CEA).
Therapy
The doctor's tactics depend on many factors.
Benign pancreatic tumors do not respond to chemotherapy and radio rays. Therefore, the only reliable method is surgery. Hormonal tumors (insuloma) are removed as soon as possible. After all, the release of insulin can lead to a hypoglycemic coma. Other formations (hemangioma, fibroma, lipoma) can wait. Treatment requires careful preparation and an accurate diagnosis.
If benign cells divide slowly, why perform surgery at all? After all, you can adhere to a wait-and-see approach (monitor the formation 2 times a year). In some cases this is what they do. Especially if the tumor is found in a person with severe concomitant pathology. Treatment may be delayed. However, benign cells can develop into cancer. This is especially true for cysts and leiomyomas. In addition, as a result of this process, emergency treatment is sometimes required (obstructive jaundice, intestinal obstruction, enzyme deficiency).
Treatment and the extent of the operation are determined not only by the nature of the tumor, but also by its location. In case of disease of the tail of the gland, resection can be performed - partial removal of the organ. Enucleation of a tumor without pancreas tissue is carried out for hormonal tumors and cystomas. The most difficult surgical treatment is when the disease is localized in the head of the gland. In this case, resection of part of the gland and duodenum is performed.
Modern therapy for some types of tumors allows mini-surgeries to be performed. For example, for hemangiomas, embolization of the feeding vessel can be done (artificially blocking the path for blood supply to the tumor). With ERCP, surgeons are able to take a biopsy from a pancreas formation through a probe. Moreover, the treatment does not require long-term anesthesia and opening of the abdominal wall.
Symptoms of pancreatic disease usually appear in older people. Patients with poor nutrition (high fat, low fiber), smokers, and alcoholics are predisposed to them. Oncology also develops against the background of chronic cirrhosis, liver hepatitis, and chronic pancreatitis.
Treatment of pancreatic tumors
Treatment of benign tumors is only surgical:
- distal pancreatectomy,
- resection of the head of the pancreas,
- pancreatoduodenal resection,
- tumor enucleation.
After the operation, a mandatory histological examination is carried out to clarify the type of tumor.
For malignant neoplasms, the main directions of therapy are selected based on the clinical situation.
Complex therapy for pancreatic tumors may include radiation and polychemotherapy (with a high proliferation coefficient, active hormone synthesis, malignancy and metastasis of the tumor).
Treatment method
Treatment of pancreatic tumors is carried out in special diagnostic centers, which conduct a range of studies, and the conclusion of specialists determines the further treatment regimen.
The main method is surgical intervention, depending on the location of the lesion and the type of formation that has arisen. The procedures used are discussed in more detail below.
Head resection
This operation is performed when a tumor forms in the tail of the organ and is performed as a partial resection with the removal of part of the pancreatic parenchyma. Complete excision of the head is quite difficult, since it is connected by a large number of blood vessels to the duodenum.
Enucleation
Removal of the resulting tumor by exfoliation of tissue. This procedure is performed when hormonal disorders occur (gastrinoma, insulinoma, somatostatinoma). The operation can be carried out if there are clear boundaries and dimensions of no more than 2 cm.
Contraindications are glucagonoma and the presence of chronic pancreatitis. The technique is carried out using laparoscopy (a small incision in the abdominal cavity and removal of the cavity). Recovery lasts 3–4 days, and then it is necessary to follow the therapeutic diet No. 5 with moderate physical activity.
Pancreaticoduodenectomy
Pancreatoduodenal resection involves complete excision of the head, gallbladder, part of the small intestine, stomach, and lymph nodes. This procedure is quite complex and should only be carried out by highly qualified specialists.
Indications for surgery are large benign or malignant tumors. The organs are removed sequentially and an artificial duct is created in the resulting space.
Currently reading: Treatment of the pancreas with folk remedies quickly
Gastrectomy
During gastrectomy, the stomach is completely removed and an anastomosis is formed. The operation is performed for indications such as multiple ulcers due to the development of gastrinoma. At the same time, resection of the initial section of the intestine is performed.
Selective arterial embolization
This technique is based on the introduction of a special substance that thromboses blood into the vessels of the organ, which reduces the size of the formation and prevents the development of computed angiography. The removed tumor must undergo histology.
Prognosis of pancreatic tumors
The prognosis for malignant tumors of the pancreas is extremely unfavorable, which is associated with their asymptomatic course and late diagnosis.
Radical tumor removal is possible only in every tenth patient, in every second patient the tumor recurs, and in 95% distant metastases are detected within the first 12 months after surgery. Complex therapy does not significantly improve survival rates: within five years, no more than 5% of patients with malignant tumors of the pancreatic zone remain alive.
The prognosis for benign pancreatic tumors is favorable – in nine out of ten patients a complete cure can be achieved. In addition, benign neoplasms of this location are rare.
What is endocrine pancreatic cancer
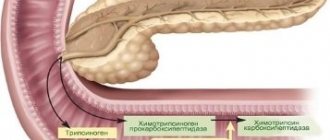
There are two types of cells in this organ:
- exocrine, which produce enzymes for processing food;
- endocrine, which produces hormones and insulin.
Neuroendocrine cancer is the proliferation of endocrine cells to form pathological tissue.
The World Health Organization (WHO) considers the increase in the incidence of this disease catastrophic.
Over 30 years, the incidence rate has increased 5 times and continues to grow. But many experts believe this increase is a consequence of improved diagnosis of the disease.
On this topic
- Oncogastroenterology
Feces for stomach cancer
- Natalya Gennadievna Butsyk
- December 6, 2020
Neuroendocrine pancreatic cancer is several types of cancer formed by endocrine pancreatic cells that grow slowly. These cells synthesize active substances necessary for digestion and the functioning of the nervous system. Their incorrect division forms NET. Not all neuroendocrine tumors are malignant.
This type of cancer is still poorly understood. The peculiarity of these tumors is that they do not give any special symptoms and are not noticed by patients until they metastasize.
Malignant tumor
Pancreatic cancer is a malignant tumor that usually develops from the epithelial tissue or ducts of the pancreas. According to histological characteristics, there are 5 main cancer forms: adenocarcinoma, cystadenocarcinoma, poscocellular, aciar cell and undifferentiated cancer. Almost 4/5 of all cases of pathology are adenocarcinoma.
A malignant tumor has a high rate of development and the ability to metastasize. According to the degree of metastasis, the following stages are divided:
- the first stage – transition to close pancreaticoduodenal lymph nodes;
- the second stage – damage to the hepatoduodenal and retropyloric nodes;
- third stage – metastases in the celiac and superior mesenteric lymph nodes;
- fourth stage - metastases reach the retroperitoneal nodes, and the hematogenous mechanism provides distant metastases (kidneys, lungs, liver, bones).
The severity of the disease is usually divided into stages:
- Stage 1A: the tumor is no more than 2 cm in size without metastases.
- Stage 1B: The tumor may be larger than 2 cm but is confined to the gland.
- Stage 2A: the tumor extends beyond the gland, but does not reach the celiac trunk and superior mesenteric artery, without metastases.
- Stage 2B: Metastases may be found in regional lymph nodes.
- Stage 3: the tumor grows in the celiac trunk and mesenteric artery, metastasis can be found in all nearby lymph nodes.
- Stage 4: distant metastases.
The main causes of cancer: hereditary and genetic predisposition, alcoholism, smoking, excessive consumption of animal fats and spicy foods, endocrine diseases (diabetes mellitus, cirrhosis). The following diseases are considered precancerous pathologies: pancreatic adenoma and cyst, chronic pancreatitis.