The appearance and proliferation of pathobacteria in the gallbladder leads to the development of a disease such as non-calculous cholecystitis. It is accompanied by painful sensations.
Manifests itself in acute and chronic forms. The acute form is characterized by a favorable prognosis, provided that medical prescriptions are followed.
Lack of proper treatment and non-compliance with recommendations leads to exacerbations.
Anatomy, functions of the gallbladder
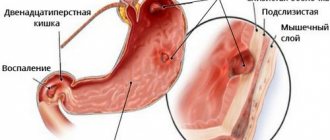
On the underside of the liver is the gallbladder. It resembles a bag eight to fourteen centimeters long and three to five centimeters wide.
In adults, the volume is about 70 cubic meters. cm. Filled with bile, which comes here from the liver.
The structure includes a wide bottom, body and neck. From the neck comes the cystic duct, which connects the organ with the bile duct.
The walls of the organ consist of the following tissues:
- connecting;
- muscular;
- epithelium.
The main purpose is the accumulation and outflow of bile. Its synthesis occurs after a person has eaten. At this time, the muscle tissue of the bladder contracts, internal pressure increases, the sphincter relaxes, bile pours into the duct and enters the intestines.
Next, bile participates in the absorption of vitamins and fats and provokes the production of pancreatic juice.
Main reasons for development
A typical mistake made by a patient diagnosed with acalculous cholecystitis is the search for one single cause that could lead to the development of an inflammatory process in the cells of a hollow organ. A good diagnostician and an experienced clinician understand that the development of calculous and non-calculous (acalculous cholecystitis) is not a process caused by one provocateur.
To launch the starting scenario, the intersection of several negative vectors in a certain segment of the body is necessary. Often they are sent from different places, at first glance, not connected with each other.
A common misconception is the lack of understanding that the human body is a single system in which all disorders are interconnected. One disease inevitably leads to another, especially when it comes to the nearby digestive and hepatobiliary systems.
Most diseases develop against the background of impaired immunity, but the cause may also be a problem in the endocrine or metabolic system, because they also take part in the breakdown, absorption and delivery of nutritional components.
Manifestations of cholecystitis are rarely differentiated according to etiological criteria, because the origin of inflammation is variable. Acute - as a separate condition, is simply called acute acalculous cholecystitis.
Permanent recurrence, which occurs due to the lack of necessary treatment not only for the gallbladder, but also for the main provoking factors, eventually turns into a chronic process, which is differentiated by the severity of symptoms - mild, moderate and severe stages of chronic acalculous cholecystitis.
The main condition for the development of any form of acalculous cholecystitis is the presence of a pathogenic agent. Despite the apparent inaccessibility and protection of the hollow organ (this is clearly noticeable during diagnostics), infection can penetrate in three ways:
- Lymphogenic, when the provoking reasons for the development of acute cholecystitis is the passage of any of the pathogens present in the body through the lymphatic system. In this way, the infection can easily develop in acute or chronic appendicitis, persistent infection in the respiratory system, or any inflammatory diseases that have become purulent. The relative frequency of development of sluggish chronic acalculous cholecystitis is often explained by inflammation of the female genital area, and in men it can occur against the background of urethritis, prostatitis and balanoposthitis of infectious origin.
- Hematogenous - a relationship has been noted between acalculous chronic cholecystitis and constantly present periodontal disease, pneumonia and infections in a permanent course. Proteus, enterococcus, or parasitic invasion from the liver through the hepatic artery can also lead to the development of the disease.
- Ascending is the most common path of development of the inflammatory process in one of the three membranes of the gallbladder, when the cause is ascending intestinal infections.
If we consider the problem globally, then it all starts with a weakened immune system, which is unable to resist the infection that has entered the body and is present there, after the acute phase, in the form of a chronic process. Lack of proper treatment leads to the spread of the pathogenic agent in the body, for which one or more transmission routes are used.
However, for the disease to develop, there must be a functional malfunction in its functioning, which is assumed to lead to liver damage. The infectious aggressor finds itself on fertile soil and takes root in its own existing focus.
The presence of long-term progression of chronic acalculous cholecystitis leads to deformation of individual organ fragments, loss of bile outflow function, and cessation of gallbladder function.
In the absence of correct treatment of non-calculous (chronic acalculous) cholecystitis, complications develop in several directions at once: negative transformations of the hollow organ itself, the appearance of polyps and growths, adhesions with nearby organs, liver diseases (reactive hepatitis), pancreas, etc.
Non-calculous cholecystitis
The most common diseases of the gallbladder include calculous cholecystitis, dyskinesia, cancer, and polyps.
One of the pathologies associated with the occurrence of an acute inflammatory process is chronic non-calculous cholecystitis. The disease is recognized by doctors all over the world. In ICD-10 it is assigned code K8 1.8.
The course is characterized by acute and chronic forms. It is diagnosed in 7 cases out of 1000, with women getting sick more often. Sometimes cholecystitis also affects children.
When the disease occurs, connective tissue grows and scars appear. Gradually, new formations replace gallbladder tissue. Peristalsis is disrupted, and the ability of the walls to contract decreases. Areas of the organ become denser, the mucous membrane becomes thinner.
The resulting inflammation in approximately 10% of cases becomes chronic.
To classify pathology, several parameters are used:
- Form. Marked as mild, moderate and severe.
- Phases. In development, there is a phase of exacerbation, reduction of symptoms, and remission.
- The nature of the current. It is noted to be monotonous, recurrent and variable.
- Manifestation. The disease proceeds in a typical form. In rare cases, it appears atypically.
The pathology is inflammatory in nature and is not associated with the formation of stones.
Classification
Typically, both types occur chronically with exacerbations of varying frequency. There is also an acute course of the disease. The acute phase, unlike the chronic phase, is easily and successfully treated. It is necessary to determine the type of disease before treatment.
Chronic acalculous cholecystitis, abbreviated as CAC, is classified based on inflammation. There are catarrhal, phlegmonous, gangrenous varieties. The presence of a complication is also an indicator. The disease is divided into complicated and uncomplicated. The disease is also classified according to its leading factor. There are postoperative factors, oxygen-free, enzymatic and ischemic.
Inflammation is divided according to the stages of its course into mild, moderate or severe and according to the nature of the course into variable, recurrent and monotonous. It also develops in a classical form and in an atypical one.
Classification of chronic non-calculous cholecystitis
Depending on the stage of inflammation there are:
- subsidence of exacerbation;
- persistent subsidence;
- unstable remission.
According to the clinical course there are:
- typical;
- atypical form.
The nature of the progression of the disease also varies:
- recurrent;
- monotone;
- intermittent.
Chronic acalculous cholecystitis can be complicated or uncomplicated.
Symptoms
The disease manifests itself in typical and atypical forms.
Typical signs
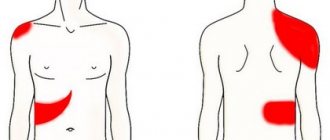
The acute form is characterized by the appearance of severe pain on the right side under the ribs. They appear after eating, especially if a person has eaten a spicy dish or drank beer. Painful sensations radiate to the shoulder and back.
Another characteristic symptom of cholecystitis is belching, accompanied by the appearance of bitterness in the mouth.
The third symptom is nausea. All three symptoms of cholecystitis of the non-calculous system usually appear after eating.
Over time, bloating, flatulence, skin rash, and vomiting appear. There is a feeling of dryness and burning in the mouth.
Patients experience an increase in irritability and a decrease in performance. Against the background of an acute form or exacerbation, the temperature sometimes rises.
As a rule, it does not rise above 37.5-37.7°C. Weakness, headaches, anxiety, malaise, and other symptoms of intoxication appear
In the subacute form, attention is drawn to a yellow tint to the eyes, skin, constipation, diarrhea, and the urge to vomit.
Atypical symptoms
Approximately a third of patients are diagnosed with chronic non-calculous cholecystitis in an atypical form according to the cardiological, intestinal and esophageal variants.
Manifestations of the cardiac form can be confused with heart disease. Pathology manifests itself in the later stages.
After eating or lying down, rapid heartbeat, arrhythmia, and pain in the chest begin.
The development of the esophageal non-calculous type is indicated by the occurrence of heartburn, discomfort when swallowing, and pain in the abdominal area.
The intestinal type is manifested by slight pain in the intestinal area, rumbling, stool disorders, and bloating. It occurs due to a deficiency of bile in the intestinal tract.
Symptoms and diagnosis
For 70% of all patients, they demonstrate a typical clinical picture, which, at the first visit to a therapist, allows one to suspect chronic non-calculous cholecystitis. Most often, patients complain of:
- Constant dull pain under the right rib or in the stomach area, which responds poorly to non-steroidal anti-inflammatory drugs. This type of pain is characterized by intensification after eating “forbidden” foods (alcohol, fried, spicy, over-salted). Typical acute colic, which occurs in patients with cholecystitis with stone formation, is not typical for non-calculous cholecystitis.
- Nausea.
- Periodic or constant feeling of bitterness in the mouth.
- Painful belching.
- Prolonged low-grade fever, accompanied by weakness and drowsiness. A rise in body temperature to febrile levels indicates necrosis of the gallbladder or cholangitis.
Sometimes, with an atypical course, patients encounter:
- heartburn;
- increased gas formation;
- constipation;
- non-localized pain throughout the abdomen.
Diagnosis of non-calculous cholecystitis is not particularly difficult. In most cases, it is sufficient to collect an anamnesis, clarify all the factors predisposing to the disease, as well as palpation, which indicates severe pain in the right hypochondrium.
To verify the diagnosis and exclude more severe pathologies (for example, cancer), instrumental and hardware techniques are used:
- ultrasonography;
- gastroduodenal intubation;
- cholecystography;
- cholegraphy;
- arteriography;
- scintigraphy.
Causes
The main cause of cholecystitis is considered to be the proliferation of pathological bacteria in the gallbladder: Escherichia coli, Proteus, enterococci, staphylococci.
It has been proven that bile is able to cope with bacteria, and the epithelium is characterized by performing local immune defense functions.
As a result, it is generally accepted that the occurrence of the disease is influenced by provoking factors:
- Stagnation of bile. This pathology is caused by the structural features of the gallbladder: the presence of compression, kinks, constrictions. It is provoked by a decrease in the tone of the muscle tissue of the bladder, associated with inflammation, psycho-emotional, and hormonal disorders. Stagnation in some cases occurs during pregnancy due to compression of the internal organs by the growing uterus.
- Eating disorder. Cholecystitis develops from overeating or from alternating hunger strikes and excessive food consumption.
- Parasitic infestations. Spread of giardiasis, opisthorchiasis.
- Deformations of the biliary system.
The development of the disease is associated with the involvement of a number of factors. Due to impaired bile output and decreased peristalsis, low-grade inflammation occurs.
When an infectious element enters this environment, the inflammatory process increases and affects the entire organ.
There are three sources of infection for non-calculous cholecystitis:
- Rising. Caused by sphincter dysfunction, biliary dyskinesia.
- Descending. The infection enters the organ through the blood through the hepatic artery and collar vein.
- Lymphogenic. It is provoked by pneumonia, gynecological diseases, appendicitis.
The classic method for diagnosing chronic cholecystitis is duodenal intubation.
During staged duodenal chromatic sounding, hypertonicity of the sphincter of Oddi is detected in 22% of patients, hypertonicity of the sphincter of Oddi is detected in 14%, and in 56% a combination of hypertonicity of the sphincters with hyperkinesia or hypokinesia of the gallbladder is detected. During duodenal intubation, the volume of portion B may be increased (more than 50-70 ml).
Microscopic examination of bile sediment is of little help to the diagnosis, since convincing criteria for inflammation usually cannot be detected due to the fact that leukocytes in the bile are quickly destroyed.
Bile culture sometimes helps to establish the etiological factor of the inflammatory process and determine the sensitivity of the microflora to antibiotics. However, the results are of conditional significance, since the contents of the duodenum are always mixed with the cystic portion of bile.
Escherichia, Proteus, streptococcus, staphylococcus and other microorganisms are cultured from the walls of the gallbladder and directly from the gallbladder bile in patients with chronic non-calculous cholecystitis. As a rule, pathogenic and opportunistic monocultures are sown. Often, in cultures of bile obtained from an inflamed bladder, there is no microbial growth at all.
The study of the physicochemical (lithogenic) properties of bile is important in the diagnosis of cholecystitis.
In chronic non-calculous cholecystitis in the acute stage, the total amount of bile acids in gallbladder bile is reduced to 70%. Most patients experience a more significant decrease in the level of tauroconjugates, which leads to an increase in the glycotaurocholate coefficient. When total bile acids decrease by 2 times, the level of tauroconjugates decreases by 4 times. Along with this, a more intense decrease in the level of glycocholic acid in bile is detected than in taurocholic acid. In most cases, there is a significant decrease in the concentration of trioxycholanic bile acids (tauro- and glyco-) and an increase in the dioxycholate-trioxycholate ratio, which indicates a decrease in the synthesis of trioxycholates in the liver. In more than half of the cases, an increased concentration of lithocholic acid is detected.
Violation of conjugation processes leads to an increase in free bile acids in bile and blood. Impaired excretory function of the liver in patients with cholecystitis is manifested by a decrease in the coefficient of extraction of cholates into bile, which leads to an increase in the level of cholates in the blood.
In patients with chronic acalculous cholecystitis, the bilirubin content in bile increases 2-3 times. In 2/3 of patients, the presence of direct bilirubin, indirect and ether-soluble bilirubin was noted in the bile. The content of phospholipids can either increase or decrease, and the content of the lipid complex can decrease.
Of the bile components of organic origin, the most characteristic for exacerbation of calculous and non-calculous cholecystitis is considered to be an increase in protein, including C-reactive protein, and glycoproteins. During the remission stage, the level of protein in bile can decrease by 1.3 times.
In patients with chronic noncalculous cholecystitis, the amount of free amino acids increases due to the inflammatory process and impaired absorption.
To diagnose inflammation in the gallbladder, the cholate-cholesterol ratio is used. In the presence of inflammation, its value is less than 6, while the norm is 9-10. It has been established that a decrease in the cholate-cholesterol coefficient makes it possible to diagnose not only severe forms of cholecystitis, but also subclinical ones.
In chronic cholecystitis, especially in the gallbladder bile, cholesterol crystals from + to ++++ are detected. The study is carried out in the bile sediment after centrifugation.
Diagnostics
The main symptom of acalculous cholecystitis is pain on the right side that occurs after eating.
The doctor listens to the patient, writes down the medical history, provoking factors, and conducts an examination.
A white tongue sometimes indicates the possible development of the disease. The appearance of this symptom is associated with stagnation of bile.
On palpation, pain appears or intensifies. The sensations become aggravated when you press the gall vertebra while inhaling, lightly hit the chest with the side surface of your palm, tap on the area of the ninth-eleventh thoracic vertebra, or press in the area where the occipital nerve passes.
Additionally assigned:
- General blood formula. The results indicate the presence of inflammation.
- Biochemistry of blood. Pathology is indicated by an increase in bilirubin, aspartate aminotransferase, and liver enzyme.
- Analysis of urine.
- Duodenal sounding. Shows signs of impaired peristalsis. Protein, acids, cholesterol, and bile are found in bile.
- Ultrasound of internal organs. When conducting this study, signs of changes in the structure of organs, wall thickness, and symptoms of a non-calculous type of inflammation are detected.
- X-ray using contrast.
- Cholescintigraphy. During the examination, the biliary system is visualized using radiopharmaceuticals, information is obtained about the functioning of the bladder, the ability of the walls to contract, the absence of obstructions in the path of bile flow, and the functioning of the sphincters.
How does the disease manifest?
Acute acalculous cholecystitis has a violent onset. Patients note the development of intense pain in the right hypochondrium, radiating to the scapula, shoulder, and lower back. The temperature rises to 380 C. Painful sensations are accompanied by thirst, constipation, increased gas production, and nausea. Characteristically, the pain intensifies with light tapping of the abdomen in the liver area.
Chronic acalculous cholecystitis provokes the appearance of pain and dyspeptic disorders. Painful sensations occur in the right side under the ribs and are characterized by an aching character. Many patients note that pain develops due to the consumption of alcoholic beverages, fried and fatty foods. Sometimes pain is accompanied by sleep disturbances and increased irritability.
Dyspeptic syndrome provokes the following symptoms of acalculous cholecystitis:
- Alternating diarrhea and constipation;
- The appearance of belching air;
- Bitterness in the mouth;
- Nausea;
- Increased gas formation;
- In the acute stage, the temperature rises to subfebrile levels.
The esophageal form of chronic noncalculous cholecystitis has the following symptoms:
- Heaviness in the abdomen;
- Frequent heartburn, which is only temporarily relieved by medications;
- Pain behind the sternum;
- Minor dysphagia.
Chronic acalculous cholecystitis sometimes occurs in the intestinal form, then patients note pain in the intestinal area, prolonged constipation, and increased formation of gases. With the cardialgic form, a person experiences arrhythmia, chest pain, and changes in the ECG.
Important! If pericholecystitis occurs against the background of chronic cholecystitis, then patients experience constant pain in the right side.
Treatment
In order to treat acute and chronic acalculous cholecystitis, medications, traditional medicine methods are prescribed, and surgical intervention is performed.
Outside of exacerbation, in the absence of symptoms of non-calculous cholecystitis, treatment with physiotherapeutic methods is indicated.
Drug therapy
Treatment with drugs includes painkillers, antispasmodics, and agents that improve the flow of bile.
- Antispasmodics are used to relieve acute pain and spasms. These are No-Shpa, Analgin, Platyfillin, Papaverine.
- In case of severe, prolonged pain and the presence of signs of inflammation in the tests, it is recommended to use broad-spectrum antibiotics: Erythromycin, Cefantral, Ampicillin.
- To eliminate signs of intoxication (vomiting, nausea), Hemodesa is prescribed intravenously.
- Enzymes will help normalize digestion. This is Festal, Mezim Forte.
- To increase bile secretion, Allohol, Cholenztm, Ursohol are used.
- Cholekinetics have a choleretic effect: Holagol, Urolesan N.
- For giardiasis, take Furazolidone.
Vitamins B and C are included in complex therapy. During an exacerbation, the patient is advised to remain in bed, table No. 5.
Surgery
The lack of effectiveness of drug treatment for non-calculous cholecystitis and the occurrence of complications are indications for surgery.
During laparoscopy, several incisions are made through which the organ is removed. An intracavitary operation is performed. Healing after such a procedure takes a long time.
Physiotherapy
During the period when cholecystitis passes the acute stage, the use of physiotherapy methods is indicated.
Cryotherapy can relieve inflammation. An abdominal massage is performed. UHF therapy has a similar effect.
Spasms are eliminated using electrophoresis using antispasmodics, high-frequency magnetic therapy, and paraffin baths.
To improve bile flow, electrical stimulation of the biliary system is prescribed. The procedure is contraindicated in case of frequent exacerbations, the presence of purulent formations, empyema, or exacerbation of cholangitis.
Mud treatments are prescribed.
Traditional therapy
In order to improve the outflow of bile, taking a decoction of Phytogepator is indicated. The mixture contains yarrow, chamomile flowers, calendula, tansy, mint leaves.
Olive oil is used to stimulate the flow of bile. Drink a teaspoon three times a day for three days.
Black radish has similar medicinal properties. Squeeze the juice from the root vegetable and drink 50 ml per day.
Treatment with rosehip decoction is indicated. The dry root is crushed and boiled in a glass of water.
To treat chronic non-calculous cholecystitis, a decoction of a mixture of immortelle, mint leaf, yarrow stem, wormwood, and fennel grains is used. It is prepared from 10 g of the mixture, filled with two glasses of cold water.
Sage, brewed in boiling water and infused for half an hour, relieves inflammation. To prepare, take two spoons of the plant and 2 glasses of water.
Treatment of chronic acalculous cholecystitis
Acalculous uncomplicated cholecystitis is treated conservatively. Therapy is aimed at:
- destruction of microbial flora in the biliary system;
- improvement of bile drainage into the intestines;
- normalization of digestion;
- pain relief.
Surgical intervention is indicated for persistent and recurrent disease, inoperability of the gallbladder and complications.
Drugs
Treatment of acalculous cholecystitis with medications improves quality of life and prevents complications. To restore the functions of the biliary system organs, medications of different groups are used:
- Antibiotics (Furazolidone, Erythromycin, Cefazolin) - kill pathogenic bacteria in the biliary system. For the treatment of non-calculous cholecystitis, broad-spectrum drugs are selected.
- Antispasmodics (Drospa, Spazgan, Papaverine) - reduce spasms in the muscles of the biliary system. They improve the patency of the bile ducts and prevent bile stagnation.
- Enzyme preparations (Enzistal, Festal, Forte Enzyme) - stimulate the digestion of food in the small intestine. Prevent fermentation and bloating.
- Choleretics (Liobil, Tanacechol, Artichol) - enhance the synthesis of bile, increase the content of bile acids in it.
- Cholecystokinetics (D-Sorbitol, Magnesium sulfate) – stimulate peristalsis of the bile ducts and bladder.
Antimicrobial drugs are selected taking into account the bacterial flora isolated from bile.
Diet
For the acalculous form of cholecystitis, you must follow dietary table No. 5, developed by Pevzner. During exacerbations, eat up to 7 times a day in small portions. The basis of the diet consists of foods rich in:
- folic acid;
- retinol;
- iron;
- cyanocobalamin;
- tocopherol.
The menu includes dietary meat, fresh vegetables, low-fat dishes:
- legumes;
- wheat bread;
- crumbly porridge;
- low fat cottage cheese;
- lettuce leaves;
- sweet apples;
- lean beef.
It is strictly not recommended to consume processed foods, fast food, alcohol and any soda. During treatment, exclude from the diet:
- spinach;
- mustard;
- tomatoes;
- salo;
- black coffee;
- sorrel;
- fatty fish;
- smoked meat;
- canned fish.
If there are no diseases of the urinary system, you should drink up to 2 liters of free fluid per day.
Operation
Surgical intervention is performed for the following indications:
- pericholecystitis;
- untreatable cholangitis;
- persistent cholecystitis;
- inoperability of the gallbladder.
In such cases, cholecystectomy is prescribed - an operation to remove the gallbladder. This is done in two ways:
- classic – open surgery with access to the gallbladder through the anterior abdominal wall;
- laparoscopic - a minimally invasive intervention in which the bladder is removed through small punctures in the abdomen under video surveillance.
In the absence of contraindications, preference is given to laparoscopic surgery. It causes complications less often. After it, no noticeable cosmetic defects remain on the stomach.
Traditional methods
Outside of exacerbations, they resort to exercise therapy, treatment with mineral waters and blind tubing. Herbal medicine is used to prevent relapses. Use herbs that have anti-inflammatory and choleretic properties:
- Chamomile. 3 tbsp. l. the herbs are steamed with ½ liter of water and left in a thermos overnight. Drink the decoction during the day, 50-100 ml per dose.
- Valerian and wormwood. Mix wormwood with valerian in a 1:2 ratio. 3-4 tbsp. l. the raw materials are boiled in 2 liters of water for 5 minutes. The filtered decoction is consumed 50 ml three times a day before meals.
- Collection of herbs. Mix 5 g of motherwort herb, mint, immortelle and St. John's wort. Boil in 1.5 liters of water for 10-15 minutes, leave for at least a day. Drink 50 ml half an hour before meals 3 times a day.
Acalculous cholecystitis is an inflammation of the gallbladder in the absence of stones. Timely treatment reduces the risk of exacerbations, so at the first symptoms of the disease you should consult a gastroenterologist.
Diet
An important part of the treatment and prevention of cholecystitis is diet. It is recommended to eat up to six times a day, with the last time two hours before bedtime.
The menu is based on reducing the consumption of fatty foods rich in cholesterol. It is recommended to exclude red meat, poultry, lard, offal, egg yolk, and butter.
Instead, for most dishes use vegetables, rabbit meat, and white lean fish. Carrots, bell peppers, dried fruits, melon, pumpkin are useful.
You need to drink up to one and a half liters of liquid per day. Drink mineral water half an hour before meals. It should be without gas.
Sweets, smoked foods, and fried foods are prohibited. Soda and alcohol are excluded. All vegetables, berries, fruits are consumed only in processed form.
All dishes must be at room temperature. Cold foods can trigger sphincter contraction.
Products that contain dyes and preservatives are removed from the menu.
Signs of cholecystitis without stone formation
The non-calculous type of disease has very characteristic symptoms. Often these signs are pronounced. With non-calculous cholecystitis, a person feels that every time in the depths of the right hypochondrium he has a dull pain after eating. Especially after fatty foods. Moreover, pain with cholecystitis radiates either to the neck, then to the shoulder or back. The second typical symptom that distinguishes a non-calculous inflammatory process in the gallbladder is belching, heartburn, and an unpleasant taste of bitterness. The third classic symptom is nausea after eating.
Other diagnostically no less important symptoms of cholecystitis, characteristic of atypical forms of the disease:
- flatulence;
- stool instability (either diarrhea or constipation);
- vomiting, often with bitter masses due to bile;
- rise in temperature;
- heart pain, tachycardia.
Non-calculous cholecystitis is finally diagnosed after laboratory tests and instrumental examination. An ultrasound helps determine whether there are stones in the gallbladder. The cholegraphy method, performed using x-rays, allows you to determine whether a non-calculous inflammatory process is developing. However, this type of examination is not prescribed during periods of pregnancy or exacerbation of the disease. Blood and stool tests are required.
Articles on the topic
- Seborrheic dermatitis of the scalp - treatment with pharmaceutical, cosmetic and folk remedies
- Choleretic drugs for bending of the gallbladder - list and types of drugs, traditional medicine recipes
- Anticholinergics - what they are and when they are prescribed, classification based on the principle of effect, contraindications
Prevention
The main way to prevent the disease is diet. However, in addition to proper nutrition, there are measures that must be followed to prevent the development of cholecystitis and exacerbations.
Among these measures:
- Regular morning exercises. It is recommended to perform special exercises to stimulate the biliary system. For example, the following: the patient lies on his stomach, grabs his ankles with his hands and bends over.
- Sports activities. Exercises should be feasible, without unnecessary stress.
- Prevention and treatment of parasitic infections.
- Elimination of stress. Try to avoid situations that cause strong psycho-emotional stress.
- Compliance with personal hygiene rules. In addition to maintaining cleanliness, it is important to empty the intestines in a timely manner.
- Avoid snacking.
- Timely treatment of diseases of internal organs.
Provoking factors
The appearance of cholecystitis is a clear example of the interconnection of all processes occurring in the human body. However, this is an equally clear demonstration of what ignoring symptoms and lack of treatment can do, even in the early stages.
The entry of a pathogen into the gallbladder does not pose any particular danger, even if it is enterococci and E. coli. Under normal conditions, they are practically powerless in the hollow organ, since this is a natural reservoir for storing bile secretions. And bile in its physiological composition has a pronounced bactericidal effect and can prevent the pathogenic activity of a pathogenic agent.
The appearance of acute inflammation and the gradual transition to a state of chronic acalculous cholecystitis begins with a change in the quantitative and qualitative composition of bile. It can be affected by a variety of factors, pathological or associated with an unhealthy lifestyle:
- sedentary work, lack of physical activity, overeating, bulimia and even pregnancy, which is natural for the female body;
- a decrease in the natural tone of the gallbladder due to endocrine diseases or inflammatory processes in the intestines (sometimes this can occur against the background of emotional instability, permanent stress);
- a common cause of a negative gallstone condition is parasitic infestations: the presence of lamblia, roundworm or amoebiasis in the body;
- the starting mechanism of acalculous cholecystitis is hormonal disorders, leading to disruptions in the digestive system, diseases of the female reproductive system, obesity, and dysfunction of internal organs;
- structural anomalies, congenital or acquired, are the result of the construction of a reservoir for digestive secretions, often leading to kinks and constrictions, compression of both the bladder itself and the ducts through which bile is transported.
Pancreatitis and hepatitis in a chronic course can be both a concomitant condition in chronic acalculous cholecystitis and can be a provocateur of the disease. Although it is possible that complications of acalculous cholecystitis will cause pancreatitis when the wall is destroyed, which has become vulnerable as a result of constantly present inflammation or a reactive process in the liver cells.
Complications
Ignoring the symptoms of non-calculous cholecystitis in adults and delaying treatment causes the following complications:
- Empyema. Foci of pus accumulation form in the cavity of the gallbladder. Severe pain, colic, and flatulence occur. The temperature rises.
- Fistula formation. Due to rupture of the walls, bile flows into the abdominal cavity, causing the development of abscesses and peritonitis. Skin color changes, nausea appears, and internal bleeding is possible.
- Hepatitis. Occurs as a secondary liver disease. It manifests itself as yellowness of the skin, sclera, enlarged liver, heaviness under the right ribs, and rapid fatigue.
- Cholelithiasis. With prolonged noncalculous cholecystitis, stones are formed from cholesterol, bile pigments, and calcium salts. Accompanied by severe pain and colic.
- Cholangitis. The inflammatory process covers the duct. Accompanied by fever, dull pain, nausea.
- Gangrene. This complication is the least common. Manifested by tissue death and pain. In some cases, vision deteriorates to the point of blindness. The temperature becomes very high. The disease often leads to death.
Based on the diagnostic results, the doctor confirms the symptoms and treatment of non-calculous cholecystitis.
Despite the fact that the disease may not manifest itself clearly, it is necessary to immediately begin taking the recommended measures. This will avoid the development of complications and exacerbations.
Main forms of the disease
Acute acalculous cholecystitis is an inflammation of the organ that develops due to the penetration of pathogenic bacteria, viruses or parasites.
The onset of the disease is characterized by a rapid onset, the patient requires urgent hospitalization in a hospital. This form of the disease occurs in 2-5% of patients with acute cholecystitis and develops in people of any age group with the same frequency in men and women. Chronic non-calculous cholecystitis is a long-term and sluggish inflammatory process that leads to fibrotic changes in the walls of the organ and disruption of its motility. The pathology is more often diagnosed in women, and the disease often develops in children. According to statistics, chronic acalculous cholecystitis develops in 10% of patients who have a history of gallbladder pathology.
Important! The chronic course of the pathology is characterized by the development of inflammatory changes in all layers of the mucous membrane of the organ, which provokes the occurrence of adhesions, abscesses, and pseudoverticula.