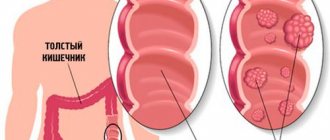
Why does intestinal obstruction develop?
The mechanism of development of the disease is associated with the appearance of obstacles that do not allow feces to move normally between parts of the intestine. There are many reasons for the occurrence of stagnation; doctors use them to determine the types of disease. Intestinal obstruction in children can be congenital (diagnosed as atresia, stenosis) or acquired.
In the first case, it is clear that the child is born with a problem. In the second, the disease develops after some time under the influence of various factors, which are divided into functional and mechanical.
The number of mechanical factors are:
- hematomas;
- helminthic infestations;
- intestinal volvulus;
- decrease in intestinal lumen;
- irregular structure of the peritoneum;
- inflammatory processes in the tract, etc.
Mechanical atresia is classified as:
Pediatrician Komarovsky classifies such pathological conditions as functional factors: spasms and paralytic phenomena, Hirschsprung's disease and disruptions in intestinal motility.
Types of disease
Blockage of certain parts of the intestine can occur in children of any age, including infants and newborns.
Main types of intestinal obstruction:
- Congenital. This type of disease occurs due to pathologies during the development of the child’s gastrointestinal system. In some cases, at an early stage of intrauterine development, congenital intestinal obstruction develops in the fetus even before birth. As a result, the baby is born with this disease. The course of the disease depends on the degree and level of obstruction. When the level of blockage is high, the newborn vomits bile. A low degree of obstruction is characterized by the presence of stool retention and gag reflexes in the child, which occur a few days after birth.
- Acquired. There are various forms of acquired disease. The most common type of disease is mechanical obstruction (intussusception). Less commonly, intestinal obstruction occurs due to the presence of adhesions. The disease is observed in small children from birth to 1 year. This type of intestinal blockage occurs suddenly and is characterized by acute pain and vomiting. Your baby's stool may contain blood and mucus.
Clinical manifestations of intestinal obstruction
Characteristic symptoms of the disease, which occurs in an acute form, are problems with the release of gases, constipation, vomiting, and abdominal pain. Symptoms such as stool retention and lack of gas in case of obstruction of the large intestine can be observed for several days. If the atresia is small intestinal, defecation occurs independently or after an enema. The absence of gas formation and bowel movements in pathology of the small intestine can be its late signs.
Pain in the abdomen is cramping in nature. The attacks coincide with the rhythms of peristalsis, and at these moments the pain becomes intense. The child is worried and tries to find a body position that will reduce discomfort. A severe syndrome produces a painful shock.
If intestinal obstruction in children develops in the small part, the body suffers from profuse, repeated vomiting. But emptying the stomach does not bring the long-awaited relief. With colonic stenosis, vomiting occurs infrequently.
There are also other symptoms that make it easier to diagnose a blockage:
- thirst;
- bloating;
- rapid contraction of the intestine in the early stages of pathology;
- stopping peristalsis as the disease progresses.
Among all the signs of obstruction, Val's symptom occupies a special place. This is swelling of the abdomen, noticeable visually and determined by palpation. The deviation is characterized by asymmetry, stability and preservation of localization.
In newborns and infants, atresia has similar symptoms with minor differences. These include bilious vomiting after feeding, bloating of the upper abdomen, grayish skin tone, weight loss due to dehydration, and fever. Symptoms of intestinal obstruction in babies under one year of age also include moodiness, restlessness, refusal to eat with a previously good appetite and normal behavior.
What are the symptoms of the disease?
Intestinal volvulus is accompanied by vivid manifestations of the clinical picture of intestinal obstruction in acute children. Unexpectedly for the child, paroxysmal pain, bloating and rejection of vomit appear in the abdominal area. The pain syndrome is so strong that the child cannot cry or even scream, he can only spin like a top.
If there is a necrotic condition of the compressed wall of the intestinal tract, the pain goes away and the child’s general condition becomes more complicated. Exhausting, incessant vomiting, which occurs if the small intestine collapses, occurs in the first moments of the presence of the disease.
Moreover, its appearance is earlier if the interference is located closer to the gastrointestinal tract. Vomit includes food debris at the initial stages, later it contains bile, and then vomit comes out with bloody impurities.
When an area of the large intestine is affected, vomiting either recedes or comes. There is a painful urge to empty the bowels, and there is bloating with gas retention. Obstruction is likely with diarrhea, in which lumps of normal stool occur. This phenomenon is repeated several times.
The reasons for the manifestation of the disorder are caused by developmental defects - when the intestine and certain areas of it narrow or lengthen, due to the presence of such an arrangement or turns of the intestine, which can cause interference in the movement of food through the gastrointestinal tract.
Harbingers of the disorder and symptoms of the disease:
- bloating (the abdomen takes on a scaphoid shape);
- vomit containing bile;
- scanty stool, there is a possibility of its absence or delay;
- no release of gases;
- maternal polyhydramnios during gestation;
- Down syndrome;
- heredity;
- small intestinal atresia;
- maternal diabetes;
- Hirschsprung's disease.
In the absence of a lumen in the colon or duodenum or in the presence of narrowings, the above list of symptoms should include the release of lumps from the rectum, where there are no admixtures of the cellular structures of the surface skin, which are present when the amniotic fluid is released, and the liquid swallowed by the resulting fetus. In the presence of normal intestinal patency, these cellular formations are appropriate as constituent elements in the meconium of newborns.
Intestinal obstruction in infants. In infants, the presence of such a disorder is specific. Intussusception in children is a condition when part of the intestine, everting, invades another intestine. A similar condition may occur in babies 5-10 months old, mainly in males. Children under 1.5-2 years of age can acquire such a pathology extremely rarely.
As a result of failure to provide timely assistance, the further course of the above-described disease is fraught with negative consequences. Isolation of a certain part of the intestine, as well as its exclusion from the digestive act, necrosis of certain areas as a result provokes a malfunction in the digestive system and metabolic processes.
A decrease in the protective function of the mucosa provokes an increase in the permeability of the gastrointestinal tract wall for pathogenic microorganisms and their metabolic products. Complicated intoxication occurs, developing into disorders such as peritonitis, sepsis, and multiple organ failure.
Interruption of the absorption process also applies to liquids. An insufficient amount of it in the blood, combined with vomiting, results in dehydration.
The progression of these phenomena is rapid, the process develops over the course of a day and is the cause of death if the patient does not go to a medical institution in the Pediatric Surgery Department.
Methods for diagnosing intestinal obstruction
Atresia is easily detected by abdominal x-ray. In newborns, the diagnostic test determines the “double bubble” with duodenal obstruction, fluid levels with low obstruction, and calcifications formed due to intestinal perforation and meconium ileus. Experts diagnose Hirschsprung's disease in newborns based on the results of irrigography and intestinal biopsy.
Prenatal diagnosis of intestinal obstruction in future newborns is carried out at 16–18 weeks of pregnancy. An anomaly is detected by the fact that an area of the developing child's intestine or stomach is enlarged. Small intestinal obstruction is best diagnosed at 24–30 weeks; the accuracy of the method results reaches 89%.
In most cases, it is not possible to recognize colonic obstruction in the fetus, since the amniotic fluid is absorbed by the mucous membrane of the tract. Important diagnostic criteria are an increase in the size of the abdomen and the absence of haustra - areas of protrusion in the colon.
Diagnosis of the disease in a child
When diagnosing, it is first necessary to carry out a direct examination of the child. Only after this can the doctor make an assumption about the cause of the disease.
We recommend: Massage for infants from 1 month
The most effective way would be to use an x-ray of the child's abdominal area. Due to this, it becomes possible to determine the specific place from which the disease originated. If there are certain difficulties in the diagnostic process, then specialists resort to a more effective type of radiography.
How is intestinal obstruction treated?
Babies born with signs of intestinal stenosis are operated on by a surgeon. There is no drug treatment for them. The essence of the intervention is to excise the damaged area and apply a colostomy if the condition is considered severe. In case of intussusception, resection is avoided. The intestines are straightened with air under x-ray control.
Dynamic obstruction, characterized by prolonged tension of the organ or complete relaxation of its walls, is eliminated through medical procedures:
- gastric lavage;
- subcutaneous administration of Proserin;
- enema with hypertonic solution;
- intravenous administration of hypertonic solution.
They get rid of helminthic infestations using cleansing and siphon enemas. For the procedure, a one percent sodium chloride solution is used. Intestinal walls, tired from increased peristalsis, are relaxed with antispasmodics.
Congenital intestinal obstruction still remains the main cause requiring emergency surgical intervention in the neonatal period. The clinical picture of intestinal obstruction in a newborn develops in the next few hours and days after birth, and in the absence of timely diagnosis and subsequent surgical intervention leads to the death of the child due to dehydration, intoxication, lack of nutrition and aspiration of gastric contents.
Epidemiology
On average, intestinal obstruction occurs in 1 in 1500-2000 live births.
Etiology
The causes of congenital intestinal obstruction may be the following: - malformations of the intestinal tube (atresia, stenosis); - developmental defects that cause compression of the intestinal lumen (ring-shaped pancreas, aberrant vessel, tumor); — anomalies of intestinal rotation and fixation (midgut volvulus, Ladd syndrome); — obstruction of the intestinal lumen with viscous meconium in cystic fibrosis (meconium ileus); - disturbance of intestinal innervation (Hirschsprung's disease, neuronal dysplasia).
Based on the level of location of the obstacle, high and low intestinal obstruction are distinguished; each of them has a characteristic clinical picture.
High obstruction is caused by obstruction at the level of the duodenum and the initial parts of the jejunum, low - at the level of the distal parts of the jejunum, as well as the ileum and colon.
Duodenal obstruction
Epidemiology
The detection rate averages 1 case per 5000-10,000 live births. In 30% of cases it is combined with Down syndrome.
Etiology
Considering the anatomical features of the duodenum, obstruction of this section can be caused by the following reasons: stenosis, atresia, compression of the lumen by abnormally located vessels (preduodenal portal vein, superior mesenteric artery), embryonic cords of the peritoneum (Ledd syndrome) and annular pancreas.
Prenatal diagnosis
Fetal ultrasound visualizes the dilated and fluid-filled stomach and duodenum in the upper abdominal cavity - a symptom of a double bladder, which, in combination with polyhydramnios, makes it possible to establish a diagnosis as early as 20 weeks of pregnancy.
If parents decide in favor of prolonging pregnancy, then in case of severe polyhydramnios, it is advisable to carry out therapeutic amniocentesis in order to prevent premature birth. Early diagnosis is extremely important: genetic counseling and fetal karyotype testing are required, since in 30% of cases this diagnosis is combined with Down syndrome.
Syndromology
When establishing a prenatal diagnosis of duodenal atresia, a comprehensive examination of the fetus is indicated, since in 40-62% of cases combined anomalies are possible. Among them, the most common are congenital defects of the heart and genitourinary system, defects of the gastrointestinal tract and hepatobiliary system. In addition, duodenal atresia can be part of a number of hereditary syndromes, among which should be Fanconi pancytopenia, hydantoin syndrome, Fryns, Opitz G, ODED syndromes (oculo-digito-esophageal-duodenal syndrome - syndrome of the eyes, limbs, esophagus, duodenum ), Townes-Brocks and TAR (thrombocytopenia with absent radius).
In addition, heterotaxy and the above-mentioned VACTER association have been described in duodenal atresia. Particular attention should be paid to prenatal karyotyping in duodenal atresia, since chromosomal abnormalities have a probability of 30-67%. Most often - Down syndrome. Familial cases with presumed autosomal recessive inheritance have been described.
Intrauterine diagnosis of duodenal atresia informs the neonatal team doctors in advance about the birth of such a child and allows them to organize emergency care for a sick newborn. If congenital intestinal obstruction is suspected, immediately after birth, a tube is inserted into the child’s stomach to decompress the gastrointestinal tract and prevent aspiration syndrome, enteral load is excluded, and the newborn is transferred under the supervision of a pediatric surgeon.
Clinical picture
Symptoms of high intestinal obstruction are detected already in the first hours after birth. The earliest and most persistent signs are repeated regurgitation and vomiting, and there may be a slight admixture of bile in the gastric contents. By installing a nasogastric tube immediately after birth, a large amount of contents (more than 40.0-50.0 ml) is evacuated from the stomach; subsequently, the liquid continues to flow passively through the tube. An inconsistent, but characteristic symptom is bloating in the epigastric region, in other parts the abdomen is sunken. Immediately after vomiting, bloating decreases. Palpation of the abdomen is painless. Obtaining meconium during a cleansing enema indicates partial intestinal obstruction or obstruction above the papilla of Vater, judging by the unimpeded flow of bile into the distal parts of the intestine. Together with gastric contents, the child loses a large amount of potassium and chlorides. Without treatment, dehydration quickly occurs. The child becomes lethargic, adynamic, physiological reflexes are reduced, the skin becomes pale and marbling, and microcirculation deteriorates.
Diagnostics
X-ray examination is used to confirm the diagnosis. For diagnostic purposes, direct radiography of the abdominal cavity is performed in a vertical position, on which two gas bubbles and two fluid levels are determined, corresponding to the distended stomach and duodenum. For most patients, this test is sufficient to make a diagnosis. In doubtful cases, the stomach is additionally filled with air or a water-soluble contrast agent, and the contrast accumulates above the obstruction zone.
Treatment
In case of high intestinal obstruction, the operation is performed on the 1st-4th day of the child’s life, depending on the severity of the condition at birth and concomitant diseases.
Forecast
Mortality is determined by the severity of combined malformations. In the long-term period, complications such as megaduodenum, duodeno-gastric and gastroesophageal reflux, peptic ulcers and cholelithiasis are noted in 12-15% of observations. Overall, the prognosis is favorable, with survival rates exceeding 90%.
Small bowel atresia
Congenital anomalies of the small intestine in most cases are represented by atresia.
Epidemiology
Occurs with a frequency of 1 in 1000-5000 live births. The distal ileum is more often affected - 40%, and the proximal and distal jejunum - in 30 and 20% of cases, respectively; obstruction of the proximal ileum is less common - 10%.
Prenatal diagnosis
Small intestinal obstruction in the fetus is visualized as multiple dilated intestinal loops, with the number of loops reflecting the level of obstruction. An increase in the amount of water and multiple dilated loops of the small intestine, especially with increased peristalsis and floating particles of meconium in the intestinal lumen, suggest small intestinal atresia.
Syndromology
There are combined malformations, mainly of the gastrointestinal tract (Hirschsprung's disease, additional areas of intestinal atresia, anomalies of the anorectal region) and urinary tract. Most cases of small intestinal atresia are sporadic. Unlike duodenal atresia, chromosomal aberrations are rare in small atresia. Prenatal karyotyping can be avoided because the frequency of chromosomal abnormalities in this defect is low. When pregnancy is prolonged and severe polyhydramnios is present, therapeutic amniocentesis is indicated to prevent premature birth.
Helping a newborn in the delivery room
Intrauterine signs of congenital obstruction of the small intestine in the fetus require organized action by the maternity hospital staff. A low level of obstruction causes a significant increase in the volume of the abdomen, which draws the doctor’s attention already at the initial examination. When inserting a gastric tube, a large amount of content is obtained, often stagnant in nature with an admixture of dark bile and small intestinal contents. The absence of meconium during a cleansing enema confirms the suspicion; an emergency transfer of the child to a pediatric surgical hospital is required.
Clinical picture
The child’s behavior in the first hours after birth does not differ from healthy behavior. The main sign of low intestinal obstruction is the absence of meconium. When performing a cleansing enema, only impressions of uncolored mucus are obtained. By the end of the first day of life, the child’s condition gradually worsens, anxiety and painful cry appear. Intoxication phenomena quickly increase - lethargy, adynamia, gray-earthy coloration of the skin, impaired microcirculation. Uniform bloating of the abdomen progresses, with intestinal loops contouring through the anterior abdominal wall. There is vomiting of stagnant intestinal contents. Upon examination, the abdomen is soft, accessible to palpation, painful due to overstretching of the intestinal loops. The course of the disease can be complicated by perforation of an intestinal loop and fecal peritonitis, in which case the child’s condition sharply worsens and signs of shock appear.
Diagnostics
Direct plain radiography of the abdominal cavity in an upright position demonstrates significant dilation of the intestinal loops, increased uneven gas filling and fluid levels in them. There is no gas filling of the underlying parts of the abdominal cavity. The more loops are visualized, the more distal the obstacle is located.
Treatment
A newborn with signs of low intestinal obstruction requires emergency surgical treatment. Preoperative preparation can take place within 6-24 hours, which allows for additional examination of the child and elimination of water and electrolyte disturbances. Preoperative preparation should not be prolonged due to the high risk of complications (intestinal perforation and peritonitis). The goal of surgery is to restore the integrity of the intestine while possibly maintaining its maximum length.
Forecast
The survival rate of patients with uncomplicated small bowel atresia is close to 100%. Mortality is caused by complications and unfavorable background such as prematurity, intrauterine growth retardation, intestinal perforation or volvulus, and cystic fibrosis of the pancreas.
Atresia and stenosis of the colon
Epidemiology
This is the rarest type of intestinal atresia: it occurs in no more than 1 in 20,000 live births. Lesions of the transverse colon and sigmoid colon are most often observed. Colon atresia occurs in less than 5% of all intestinal atresia cases.
Prenatal diagnosis
Obstruction of the colon in the fetus can be suspected if dilated loops of the colon filled with hypoechoic contents with inclusions are detected. However, in most cases, this pathology is not diagnosed prenatally due to the resorption of fluid from the intestine and uniform expansion of the intestine throughout - without areas of significant increase in diameter. When dilated loops of the colon are detected, the differential diagnosis should be made with Hirschsprung's disease, anorectal pathology, megacystis-microcolon-intestinal hypoperistaltic syndrome and meconium peritonitis.
Intestinal obstruction in newborns is a fairly common occurrence. Sometimes a child has abdominal pain, but after stroking the tummy it goes away.
But in some cases, abdominal pain is a symptom of intestinal obstruction, which requires serious treatment.
This article discusses cases of intestinal obstruction in newborns, methods of its treatment, as well as signs that indicate problems in the intestines.
Causes
All causes of intestinal obstruction in an infant should also be divided depending on the level of damage to the digestive tract. The following forms are distinguished:
- High intestinal obstruction;
- Low intestinal obstruction.
| High | Low |
|
|
Such malformations are associated with Down syndrome in 50% of cases, therefore, in the antenatal period, primary diagnostics (ultrasound of the fetus) is mandatory.
Intussusception
There is a mixed variant of intestinal obstruction in infants, which is characterized by the penetration of the proximal into the distal. The mechanism of this disease is associated with impaired peristalsis. The hypermotility of the circular layer of the muscles of the wall of a hollow organ is of decisive importance.
The following risk factors may lead to this:
- Sudden changes in the baby’s routine/diet;
- Incorrect introduction of complementary foods;
- Lack of treatment for inflammatory bowel disease.
With the small intestinal variant of intussusception, the onset of necrosis should be expected after 12-24 hours, in the ileocolic - 6-12 hours, with localization in the colon - 36-48 hours.
Pyloric stenosis
The origin of pyloric stenosis is still unclear. The morphological substrate of the disease is the presence of a sharply thickened muscular layer of the pyloric part of the stomach, which causes a delay in evacuation and obstruction.
Statistically, it is more common among boys in the first year of life. Moreover, the clinical picture begins to develop by 3-4 weeks. At first, frequent regurgitation occurs, “vomiting like a fountain.” The child is not gaining weight and dehydration is progressing.
Timely surgical treatment allows you to quickly return the baby to normal life - by 7-8 days there are no longer any signs of digestive disorders, and weight gain begins.
There is no mortality during treatment.
Meconium ileus
An infant with cystic fibrosis may experience obstruction of the terminal ileum with excessively viscous meconium. The condition begins to develop in utero, so it can be detected by ultrasound examination.
Seeing a doctor is mandatory, since meconium ileus can cause torsion, which is dangerous due to the development of acute intestinal ischemia (infarction) and subsequent peritonitis.
Children with a family history of cystic fibrosis are at risk.
Read more about obstruction and its causes
Obstruction is divided into chronic and acquired, which can develop in two cases:
- due to intestinal compression (strangulation);
- if the anus is closed by any tumor or neoplasm (obstructive).
Obstruction is also divided into partial and complete. In the first type, the obstruction is incomplete, i.e., a small part remains for passage. In the second case, the intestine becomes completely obstructed.
In infants, the main reasons that can cause obstruction are pinched or strangulated intestines. Another name for this phenomenon is intussusception.
In this case, part of one intestine enters the area of another. In boys, after six months of life, this phenomenon occurs more often.
The cause of intestinal volvulus is disturbances in the functioning of peristalsis, which children are susceptible to.
Problems in contraction of the intestinal walls may be due to excessive mobility of the colon and immaturity of the digestive system, or a tumor in the intestine may compress the intestine.
In addition, intussusception may occur due to adhesions in the child's abdomen after surgery. If the child is quite active, the intestines may wrap around the commissure during the jump.
Problems with intestinal patency in a child also consist in stool that is too tight for the newborn’s body.
As a result, the child’s feces block the intestinal lumen, which forms coprostasis, which causes obstruction.
Coprostasis can be observed with various congenital intestinal defects. However, not only an abundance of feces, but also worms, as well as some kind of neoplasm, can block the anus.
In the case of worms, additional intestinal spasm occurs from the toxins they secrete. In such cases, treatment begins with relieving intestinal spasms.
It happens that during the first two weeks of the child’s life, profuse vomiting and nausea appear.
This can occur due to a narrowing of the sphincter between the stomach and intestines (pyloric stenosis), which prevents milk from reaching these organs.
Birth defects that can cause obstruction in a child’s body include incorrect location and size of the intestines, and incorrect location of neighboring organs (pancreas).
Lack of potassium in the blood can also cause dynamic intestinal obstruction in a newborn baby.
The development of obstruction occurs due to impaired intestinal motor function. All this is possible after surgery, pneumonia or a child’s birth injury.
Also, this deficiency of the gastrointestinal tract is possible if the newborn is sick with an intestinal infection.
So, let's summarize the causes of intestinal obstruction:
- neoplasms, tumors in the intestines;
- chronic gastrointestinal defects;
- pinching, clamping of the intestine;
- adhesions in the intestines;
- complications after surgery;
- complication after a course of medication;
- coprostasis.
Causes
differ in children under one year of age and in older children .
In newborns, the causes of this disease are disturbances in the formation of certain internal systems during intrauterine development.
The diagnosis of intestinal obstruction in most cases is made in the first days after the birth of the child.
In older children, the pathological process develops against the background of certain diseases , the consequences of exposure to negative external factors or genetic predisposition.
The following factors can cause intestinal obstruction
- excessive use of certain medications;
- serious errors in nutrition;
- congenital instability of the intestines;
- damage to the body by worms and parasites of other categories;
- progression of tumors in the digestive system;
- entry of foreign bodies into the esophagus;
- volvulus;
- intussusception (prolapse of part of the intestine in infants);
- congenital abnormalities of internal organs;
- progression of inflammatory processes in the body;
- disruption of the biliary tract;
- development of adhesive processes in the gastrointestinal tract;
- consequences of surgical intervention in the abdominal organs.
How does intestinal dolichosigma manifest in a child? Find out about this from our article.
Signs of the disease and its diagnosis
The signs of intestinal obstruction in a child are completely different. One of them is not having bowel movements after birth or passing bloody stools.
Loose stools and bloating from accumulated gases are possible. Intestinal bloating is also characteristic. In some cases it is visible to the naked eye.
In addition, a sign of obstruction is vomiting, which occurs some time after eating.
As a rule, the amount of vomit is much greater than the volume of milk that the child drank. After the stomach expands, the nausea interval may temporarily increase.
The main symptoms also manifest themselves externally - the child becomes restless, he experiences active sweating and pallor. In this case, quick and effective treatment is necessary.
Absence, delayed bowel movements and sudden abdominal pain are the main symptoms of obstruction. As a rule, the pain is expressed in the abdominal area, it occurs suddenly, in contractions, and repeats every ten minutes.
The reasons for this lie in the fact that the intestines try to push the contents through, later the pain becomes constant because the intestinal muscles get tired.
The pain may improve on the second or third day, but this is not a good sign.
Despite the symptoms that appear, it is quite difficult to diagnose “obstruction”.
It is even more difficult to clarify its type and causes, because, despite the fact that X-rays exist, it is not difficult to confuse intestinal obstruction with anything else, since similar symptoms and disorders in the intestines occur in premature babies.
However, if you suspect any intestinal obstruction, you should immediately consult a doctor, as the problem is very serious and can be fatal.
First, the doctor examines the child to determine his overall health. An X-ray examination is then possible, which can reveal defects in the development or location of the gastrointestinal tract.
Sometimes the child's intestines are filled with air or barium is used to open the intestine further to see possible tumors or coprostasis.
This procedure is done if the parents contacted no later than twelve hours after the first symptoms appeared.
In more complex cases, a special method of surgical intervention is used - laparoscopy to examine intestinal volvulus and adhesions.
It is possible to use ultrasound, but only as an additional diagnosis in controversial cases.
Diagnostics
X-ray examination helps the doctor make the correct diagnosis.
- Interviewing the child (if possible by age) and parents: allows you to find out the time of onset of the disease, complaints, the dynamics of the disease, the individual characteristics of the child’s body.
- The examination makes it possible to assess the general condition of the child, identify abdominal pain and its location, bloating, the nature of vomit and stool (if any), tension of the abdominal muscles, the state of the cardiovascular and respiratory systems, etc.
- With the help of an X-ray examination, it is possible to carry out an early diagnosis of intussusception, confirm the presence of pyloric stenosis, elongation of the sigmoid colon, etc. According to the doctor's decision, in some cases, air is pumped into the intestine through the rectum, and in some studies barium is used.
- In cases that are difficult to diagnose, laparoscopy is used (for adhesive obstruction, torsion, etc.).
- Ultrasound of the abdominal organs is used as an auxiliary examination method.
Pathology therapy
If your child experiences the above symptoms, you should immediately consult a doctor.
Intestinal obstruction in children can have serious consequences, including the death of the child.
In such cases, there is no need to self-medicate; treatment is required under the supervision of an experienced doctor.
You should contact a clinic or hospital as soon as possible, and in some cases a consultation with a surgeon may be necessary.
When the intestine volvuls, they try to straighten it with air, which is released into the child’s anus.
To be sure that the intestines have returned to normal, the baby is left in the hospital for further observations. Later, the child is injected with a barium suspension into the intestines.
If the intestine has returned to its normal state, then the suspension will be released along with the feces in about three hours.
The intestines can be straightened in this way if you seek help and begin treatment no later than 24 hours from the onset of the first symptoms.
If the obstruction is caused by a ball of worms in the intestinal lumen, then first they try to relieve the spasm from the intestine.
If this does not help, then surgical intervention is required - the surgeon cuts the stomach and tries to push the worms further through the intestines.
In some cases, if this method does not work, the intestine is cut and the worms are removed, followed by suturing.
Dynamic obstruction requires longer and more serious treatment, as well as mandatory hospitalization.
The child is given various types of enemas, the lack of potassium in the body is compensated, Proserin is injected and droppers are placed with various hypertonic solutions.
In addition, treatment of dynamic obstruction involves inserting a probe into the stomach and further bowel cleansing procedures.
Adhesive intestinal obstruction is the most dangerous. In this case, surgery cannot be avoided.
If the parents went to the hospital late, the intestines may show the first symptoms of necrosis. Then the dead part of the intestine has to be removed.
For peritonitis, treatment includes various vitamins, painkillers and means aimed at general strengthening of the body.
In case of intestinal obstruction, it is important to quickly recognize the signs and symptoms of the pathology, and then begin treatment on time.
If the first symptoms of obstruction appear in the maternity hospital, then the child is given gastric lavage and various IVs are placed.
If the condition worsens, a surgical method must be resorted to.
If there is a slowdown in the process of fecal excretion or its complete cessation, doctors say that intestinal obstruction in children has been diagnosed. The disease is complex and multi-causal. The disorder is caused by congenital malformations of the intestinal region, motor dysfunction of the organ, and growing tumors. The pathology requires immediate medical intervention, since there is a high risk of developing severe consequences, including the death of the child or newborn. The disease is treated with medication, diet therapy, and surgery.
Treatment
Before starting therapy, you will need to undergo diagnostics to confirm the suspicion of a specific disease and determine its type. Adhesive intestinal obstruction in children will be treated in a specific way, and different measures may be prescribed for each type. For diagnosis, a number of procedures are used to determine the type of disease.
- The first step is a physical examination , during which the doctor asks about your medical history and symptoms. The doctor will feel the baby's belly and make an assumption about a possible problem. If the abdominal cavity is swollen, tender and a lump is palpable, then a blockage may be suspected. Additionally, the doctor will listen to the sounds made by the abdominal area.
- X-rays can confirm the diagnosis, so if intestinal obstruction is suspected, the doctor should insist on taking a picture. Not all obstructions can be seen with regular X-rays, so a CT scan will be helpful. An ultrasound examination is often prescribed if a child has intestinal obstruction.
- The preferred measure is a barium or air enema , because this procedure can remove the pathology and eliminate further treatment. During this procedure, liquid barium or oxygen is injected into the large intestine through the rectum.
If intestinal obstruction is confirmed, the child is hospitalized after the first examination. Therapy will begin immediately to reduce the likelihood of intestinal strangulation. A number of actions will need to be taken to help improve the child’s condition.
Therapeutic measures
- First of all, a nasogastric tube will be inserted, with which the gastrointestinal component can be eliminated.
- Intravenous fluid is administered to prevent dehydration and correct ionic imbalance.
- When inversion occurs, a rectal tube is used - it is inserted into the intestines. A barium enema helps with intussusception in 70% of cases.
- Complete obstruction is eliminated through surgery. The affected area is removed surgically, and a portion of the intestine is also removed. When the problem is caused by hernias, adhesions, polyps and tumors, they are removed during surgery.
- Antibiotics are prescribed before and after surgery to prevent the risk of infection in the area of the blockage.
After taking therapeutic measures and eliminating the problem, you must follow a diet. The diet must be high in fiber so that stool can form properly.
The prognosis for many children is positive if treatment is timely. With the right approach, you can recover without complications. In only 1-2% of children, treatment does not help and death occurs.
Uncontrolled obstruction also leads to death, because quite rarely the pathology goes away without therapeutic measures.
Description of the pathology
Intestinal obstruction in children is a pathology associated with a failure in the process of pushing chyme (broken down food with digestive juice) through the lumen. In babies of the first year of life, the disease is accompanied by severe pain, cramps, and vomiting. Most people use surgical tactics to eliminate pathology, especially in newborns. Older children are prescribed conservative treatment and diet.
In infants, the disease causes severe cramping pain.
Children's intestinal obstruction is a kind of blockage of the lumen. The complexity and severity of the disease depends on the location of the problem - the higher the blockage occurs, the more severe the disease will be. The peculiarity is the manifestation of specifically rapid symptoms in a vivid form. Correct and timely response in the form of treatment determines the outcome. If the chronic form is eliminated with medication, then the acute form can only be eliminated surgically.
Classification of intestinal obstruction in children
Intestinal obstruction in newborns and older patients is classified according to genetics, anatomical-physiological, and symptomatic parameters. Correctly determining the type of blockage allows you to prescribe adequate treatment and adjust the intensity of the measures taken. International classification:
- Based on origin, a distinction is made between congenital and acquired forms.
- According to the mechanism of formation - mechanical, dynamic.
- According to the characteristics of the symptoms - complete, partial, acute, chronic.
- According to the nature of compression of the vessels supplying the intestine with blood - strangulation, obstruction, mixed (with adhesions).
Congenital
The formation of intestinal obstruction can begin in the womb.
This form of intestinal obstruction is formed in the womb against the background of fetal development abnormalities, so the newborn suffers from severe symptoms of dysfunction from the first hours. When the disease is particularly severe, the baby develops vomiting of bile and bloating. In mild forms of the disease, constipation and vomiting are observed. If this pathology is detected late, the risk of intestinal rupture increases. Manifestations of congenital pathology are stenosis (narrowing of blood vessels, lumen), atresia (fusion of organ walls), and inflammation. This form is typical for newborns.
Acquired
Pathology is provoked by external or internal unfavorable factors. It most often develops in infants aged from 4 months to a year in the form of intussusception (penetration of one part of the intestine from another) or a mechanical disorder. Adhesions are formed quite rarely. The characteristic features of the disease are an unexpected, paroxysmal pain syndrome that progresses to vomiting, and blood and mucus are found in the stool. A childhood illness requires immediate hospitalization of the baby.
The main cause of obstruction is stagnation of feces against the background of weakness (atony) of the intestinal muscles, and, consequently, peristalsis.
Dynamic
Jumps in intestinal pressure provoke peritonitis.
The development of this form is provoked by weakening of the regional blood supply to the mesentery, disruption of water and electrolyte balance, and dysfunction of the central nervous system departments responsible for correcting the functioning of the gastrointestinal tract. As a result, inflammation develops. The incidence is 10% of all recorded cases. Classification into subforms:
- paralytic, when the problem of atony arises against the background of the operation and is accompanied by paresis, a jump in intraintestinal pressure, which is fraught with intestinal rupture and peritonitis;
- spastic pathologies, characterized by excessive muscle tension, paroxysmal abdominal pain, absence of a jump in temperature, bloating, but vomiting is possible.
Mechanical
This pathology can be caused by the formation of adhesions in the body against the background of improper wound healing after intervention in the abdominal cavity. Depending on the causative factors, there are the following subforms:
Each of the listed types of intestinal obstruction in infants and older children has characteristic symptoms, but there are common signs of pathology, such as:
Intestinal obstruction in a child: symptoms of the condition in newborns and older children. Severe abdominal pain can be life-threatening.
Classification
Depending on the time of formation, the pathology can be congenital or acquired. The first option is formed during intrauterine development. Pathology can manifest itself in the form of narrowing of the organ lumen, fusion or inflammatory processes. The acquired form develops against the background of deterioration of peristalsis with subsequent stagnation of chyme.
Depending on the pathogenesis (mechanism of formation), the syndrome can be mechanical or dynamic. The first form develops against the background of adhesions, intussusception, surgical interventions, as well as compression by tumors, parasites and foreign bodies. It, in turn, is divided into strangulation and obstruction types.
With obstruction, or blockage, the intestinal lumen is compressed by fecal stones, tumors, etc. Strangulation obstruction develops against the background of circulatory disorders. It can cause peritonitis and necrosis of the intestinal wall. The causes of dynamic obstruction are associated with impaired blood circulation, central nervous system, and water and electrolyte balance. It can be paralytic and spastic.
High obstruction is diagnosed if the affected area is in the small intestine. Low – if the pathological process is localized below the bauhinium valve of the small intestine. Depending on the course of the process, CI can be acute or chronic. In childhood, the first option most often occurs. The syndrome can also be complete or partial. With a partial variant, the tone of the intestinal wall is disrupted. The full version requires immediate treatment and is life-threatening for the child.
The syndrome causes pain and bloating
Briefly about what intestinal obstruction means in children
Intestinal obstruction in a child is a condition that is characterized by stopping the passage of stomach contents through the intestines. Mechanical obstruction occurs when the intestinal lumen is closed (there is some kind of obstruction). As well as paralytic obstruction, when the intestinal muscles are completely relaxed or, on the contrary, they spasm, in this case we are talking about spastic obstruction.
During normal operation, the intestines contract and move their contents towards the exit. By its contraction we mean peristalsis. If it is broken, then problems arise.
Causes of intestinal obstruction in a child
Intestinal obstruction in children can have a number of causes. Fecal stones, immaturity of the digestive system, early complementary feeding of the baby, tumors, polyps, foreign body entry and infection can create obstacles to further transportation of intestinal contents or stop it completely.
Intestinal obstruction in newborns may be congenital. This pathology is associated with inferiority of the digestive tract. There are many birth defects, we won’t go into them here. Let's leave this to medical specialists; it is difficult for parents to understand, so we will not delve into complex medical terms and subtleties. This article is for parents for informational purposes in order to have an idea of the problem, understand its seriousness and know the symptoms.
Useful articles: