A postoperative hernia of the anterior abdominal wall means a protrusion in the area of the postoperative scar as a result of a defect in the muscle-tendon frame of the abdominal wall. There are also other names for this pathology: ventral or cicatricial hernia. The contents of the hernial sac can be the omentum, intestinal loops that move under the skin, forming a noticeable formation.
The localization of hernias of this type depends on the location of the previous surgical intervention: the area of the white line of the abdomen, the iliac or subcostal region, etc. This pathology occurs in 10% of patients who have previously undergone surgery. In half of the patients the disease occurred within a year after surgical treatment, in the rest - within five years after surgery.
Methods for diagnosing postoperative hernia
- examination by a surgeon;
- radiography of the stomach and duodenum;
- gastroscopy (EGD, esophagogastroduodenoscopy)
- herniography is an x-ray method that involves introducing a special contrast agent into the abdominal cavity to examine the hernia;
- Ultrasound of hernial protrusion;
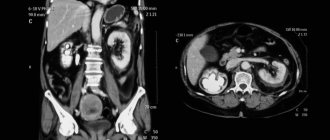
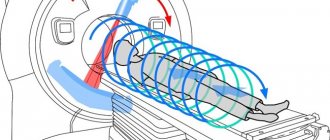
- computed tomography (CT) of the abdominal organs.
Diseases with similar symptoms
- umbilical hernia;
- hernia of the white line of the abdomen.
Treatment
In the surgical treatment of postoperative hernias, specialists perform both laparotomy (the abdominal cavity is cut) and a more gentle procedure - laparoscopy. During surgery, patients undergo hernioplasty, in which the hernia sac is removed and the hernia orifice is repaired. In parallel, the contents of the hernia are immersed into the abdominal cavity, and all weak points are strengthened using special artificial (they are used only in the medical industry) or natural materials.
The use of synthetic materials (mesh) during surgery can significantly reduce the number of relapses of this disease. This material takes root very well in the human body, and its presence does not cause any side effects in patients. Within six months, after surgical removal of a postoperative hernia, the artificial mesh completely grows into the patient’s tissues.
Thanks to such a strong frame, patients very quickly undergo rehabilitation, go back to work and begin to lead an active lifestyle.
In the surgical treatment of small postoperative hernias, specialists use the patient’s tissue for plastic surgery. In this case, the patient can undergo a simple operation, during which he is given local anesthesia. If the patient is pregnant, she will not be allowed to undergo surgery. Aggravated chronic diseases that require long-term therapy may also be a contraindication to surgery.
For this category of patients, doctors will prescribe (until the moment when surgery can be performed):
- medical supplies;
- wearing special underwear;
- lack of physical activity.
Course of postoperative hernia
Postoperative hernias in the early stages are reducible and are not accompanied by pain. However, with sudden straining, falling, or lifting, pain appears and the protrusion increases. As the hernia progresses, the pain intensifies, sometimes becoming cramping in nature. At the same time, intestinal lethargy, constipation, flatulence, nausea, belching develop, the activity of patients sharply decreases, fecal stagnation, accompanied by intoxication, is periodically observed.
Diagnostics
To diagnose postoperative pathology, a visual examination of the patient is performed. The doctor notices a protrusion in the area of the scar and performs palpation, determining the size of the protrusion, the presence or absence of pain, and the possibility of reducing the contents of the hernial sac into the peritoneal cavity. Then the patient is examined using the following instrumental diagnostic methods:
- gastroscopy;
- radiography;
- computed tomography;
- herniography;
- Ultrasound.
Thanks to these methods, doctors receive accurate information about the shape of the bulge and its size, the presence or absence of adhesions inside the peritoneal cavity.
Complications of postoperative abdominal hernia:
- strangulation - sudden compression of the hernial contents in the hernial orifice;
- coprostasis - stagnation of feces in the large intestine.
Emergency care is required if a postoperative hernia is strangulated and the following symptoms appear:
- nausea, vomiting;
- blood in the stool, lack of bowel movements and gases;
- rapidly increasing abdominal pain;
- the hernia does not reduce with light pressure while lying on the back.
Postoperative hernias are successfully treated surgically. If left untreated, an irreducible hernia may form and become strangulated.
Price
The cost of treatment is influenced by many factors: the volume of intervention, the presence of complications, the method of performing the operation, etc. Therefore, the price for each patient is individual. For more detailed information you can call
Causes
The formation of postoperative hernias is associated with the load on the tissue in the scar area; with an increase in intra-abdominal pressure and muscle contraction, the connective tissue is not able to cope with the load, resulting in a defect.
Decisive factors in this case may be prolonged coughing and physical overexertion. Often the cause of a postoperative hernia is the patient’s behavior in the period after surgery: excessive physical activity, refusal to wear a bandage, etc.
- Inflammation or suppuration of the suture after surgery also leads to pathology - the scar becomes less durable.
- Obesity, diabetes mellitus, diseases of the bronchopulmonary system, digestive organs, heredity, etc.
- Low quality suture material, violation of operating technique. But performing the operation in specialized clinics makes this factor irrelevant.
- Postoperative hernias often occur if the operation was performed for emergency reasons. Lack of time for preparation, for example, correction of the state of the digestive system, leads to an increase in intra-abdominal pressure, which negatively affects the formation of a postoperative scar. Therefore, it is important to start treatment in a timely manner rather than wait for hernia complications.
Symptoms
Symptoms of an incisional hernia appear gradually. At first, this is a painless protrusion; discomfort appears only when lifting something heavy or with sudden movements. Then the pain becomes more intense, pulling at first, it gradually becomes cramping. Constipation, flatulence, urination problems, and nausea and vomiting are common. If left untreated, complications may develop, the most serious being a strangulated hernia. Without emergency assistance, even death is possible.
Diagnostics
A protrusion is visually noted, which increases with straining; intestinal peristalsis, rumbling or noise can be observed through the scar tissue. To obtain a more detailed picture, an examination is prescribed: an ultrasound of the abdominal wall is performed to determine the width of the hernia defect, the presence of adhesions, to determine the contents of the hernial sac, etc. The examination also includes a number of studies that help exclude the presence of complications: radiography of the stomach, herniography, esophagogastroduodenoscopy, colonoscopy, irrigoscopy.
Sign up for a consultation: +7 (495) 782-50-10
Causes of postoperative hernia
A postoperative hernia is a consequence of a previously performed surgical intervention. The determining reasons for its development are:
- suppuration, inflammation of the surgical suture;
- surgical errors made during the first operation;
- increased physical activity after surgery;
- violation of the regime of wearing an anterior bandage in the postoperative period;
- insufficient restorative forces and low immunity;
- obesity;
- severe cough, vomiting, constipation in the postoperative period.
Treatment of postoperative hernia
The only way to get rid of an incisional hernia is through surgery. Types of operations (hernioplasty):
1) Plastic surgery with local tissues - suturing the defect of the aponeurosis of the anterior abdominal wall. Plastic surgery with local tissues is possible only if the defect size is small - less than 5 cm. When eliminating small postoperative hernias, local anesthesia is acceptable; in other situations, the operation is performed under anesthesia.
2) Plastic surgery with the use of synthetic prostheses - covering the aponeurosis defect with a postoperative hernia with a synthetic prosthesis. There are various methods, characterized by different locations of the mesh in the anatomical structures of the anterior abdominal wall. The chance of relapse is very low. The operation is performed under anesthesia.
Signs and treatment of ventral hernia
Ventral hernia is a complication of the postoperative period during surgery with dissection of the anterior abdominal wall. This pathology can only be treated with repeated surgery; conservative measures do not provide a therapeutic effect.
What is a ventral hernia
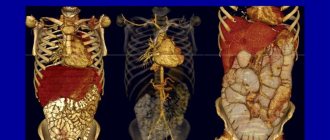
To understand the essence of the pathology, you should know the structure of the anterior abdominal wall. This is a multi-layered formation, which, when viewed from the outside, has:
- protective, outer layer dermal
- subcutaneous protective fat layer
- layer of connective tissue or aponeurotic
- muscle corset.
During abdominal surgery, all layers are dissected. A postoperative complication leading to the formation of a hernia is partial or complete divergence of the connective scar .
A ventral hernia is the prolapse (partial exit) of internal organs (omentum, small intestine, etc.) through the damaged abdominal wall into the subcutaneous area .
The outer layer of skin and subcutaneous fat holds the hernial sac, which quickly becomes overgrown with blood vessels.
As a result, the contents of the sac, the hernial orifice and the sac itself form strong adhesions (fuse together at the point of contact).
Ventral hernia is localized in the abdomen , where a cavity incision was made in all layers of the anterior abdominal wall to gain access to the internal organs. More often this happens after urgent surgical interventions, when there was no opportunity for full preoperative preparation. The hernial orifice may have several openings.
Note! Postoperative complication of this kind often occurs due to the fault of the patient himself, who is irresponsible about the recommendations of the attending physician.
Classification
There is no generally accepted classification of incisional hernias. They are distinguished:
- by localization,
- to size,
- by relapse rate.
Additionally, a distinction is made between reducible and irreducible, multi-chamber and single formations.
By localization
Based on their location, medial, lateral and combined ventral hernias are distinguished.
- Medial – located along the midline of the abdominal wall
- Lateral - hernial orifices on the sides of the abdomen
- Combined - several hernial orifices that extend from the midline to the lateral parts of the abdominal wall.
To size
Based on the size of the hernial orifice, the following types are distinguished:
- small – up to 5 cm, not visually detectable,
- average – 5-10 cm, visually looks like a small bulge on the abdomen in the area of the operation,
- extensive - 10-15 cm, noticeably deform the abdomen,
- gigantic – more than 15 cm, severe deformation of the abdomen.
By relapse rate
The characteristics of relapses of a ventral hernia directly indicate the number of its reappearances.