Main causes of cancer development
Intestinal cancer is characterized by the appearance of malignant neoplasms on the internal, mucous walls of the intestine, which later, in the absence of treatment, grows into nearby tissues and organs. The disease primarily affects adults aged 45-70 years.
The group of patients most at risk of developing cancer are people with a genetic predisposition to the disease.
Experts call the main and first motive for the growth of malignant oncology the presence of precancerous pathologies in the intestine:
- Granulomatous colitis;
- Nonspecific ulcerative colitis;
- Polyposis of the mucous layer of the colon;
- Chronic paraproctitis;
- Benign tumors: lipomas, adenomas, angiomas, etc.
Cancer can affect absolutely any organ in the human body, but the key to our health is in the intestines - that is why one of the first causes of the development of severe cancer is poor nutrition and the nature of the food consumed.
Consumption of foods low in fiber and high in preservatives, animal fats, alcohol abuse, spicy, fatty foods increases the risk of tumors.
Secondary causes of bowel cancer:
- Dysbacteriosis, accompanied by frequent and painful constipation;
- Lack of enzymes, beneficial microelements, and vitamins in the body.
- Overwork due to physical and mental stress, depression, lack of interest in life, stress;
- Smoking, frequent alcohol consumption.
What stages does bowel cancer go through?
If we consider the disease from the point of view of Russian scientists, intestinal cancer goes through 4 main stages:
- The first stage, at this time the neoplasm penetrates deeper than the submucosal part of the organ. The tumor is mobile and compacted; upon visual examination, it is sometimes diagnosed as an ulcer, since obvious intestinal erosion is visible. There are no metastases or damage to the lymphatic system.
- At the second stage, the tumor penetrates the muscle layer, sometimes reaching the serous part. The size of the tumor is ½ -1/3 of the size of the intestine. Its growth can occur in the lumen of the intestinal tract or deep into the muscular layer; it is often called hyperplasia (intestinal). In the first case, such growth is called exophytic, in the second, endophytic.
- The third stage is characterized by damage to the nearest lymph nodes, there are no metastases to organs. At this stage, a person begins to experience severe symptoms. The size of the tumor is 30-50% of the size of the intestine.
- At the last fourth stage, metastases occur that penetrate into distant organs.
Metastasis
In most cases, metastases penetrate the liver area. In addition, metastasis of the lymph nodes in the space behind the peritoneum and in the abdominal cavity itself is often detected. As the disease progresses, the lungs, ovaries, adrenal glands, pancreas, organs located in the pelvis, and bladder are affected. Depending on where the metastases have penetrated, intestinal cancer manifests itself - its signs and symptoms will be completely unexpected.
If metastases penetrate the liver, the prognosis will depend on the stage of their damage and the number of metastases
The general condition of the patient is of no small importance. Half of people with such manifestations of cancer live on average a little more than six months. With a single liver metastasis at stage 4 of the disease, the prognosis is more favorable, such people live on average 2-2.5 years
And only 1% of patients are able to live 5 or more years with a similar diagnosis.
General symptoms
Clinical manifestations of intestinal cancer are variable. Signs of the disease largely depend on the location and size of the formation. The first symptoms of intestinal cancer are nonspecific, i.e., they cannot accurately determine the presence of oncological pathology.
First, toxic-anemic signs appear, which are considered symptoms of damage to the intestinal mucosa. This causes the formation of organ defects through which infection penetrates, and harmful substances enter the blood through damaged capillaries, which leads to general intoxication of the body, expressed by such manifestations as:
- headache;
- fast fatiguability;
- aches and pains in the joints;
- anemia;
- decreased appetite;
- decrease in hemoglobin level;
- blood thickening;
- pallor of the mucous membranes;
- leakage of blood into stool.
In the future, as the malignant tumor grows in the large intestine, symptoms of inflammatory damage to large areas of the mucous membranes of the organ may appear. In this case, the symptoms of general intoxication are supplemented by various disorders of intestinal function, including the following:
- elevated body temperature (more than 38 °C);
- bloating;
- increased gas formation;
- impurities of pus, blood or mucus in the stool.
When the tumor grows into the lumen, symptoms of intestinal obstruction begin to appear. Abnormal bowel movements may indicate bowel cancer. Constipation cannot be eliminated even by using enemas and laxatives. The patient complains of a feeling of heaviness in the abdomen and rumbling in the intestines as the cancer progresses.
Symptoms of the pathology worsen after eating, especially if it is difficult to digest. In the later stages of the pathological process, dyspeptic disorders increase. Constipation and diarrhea become common, which indicates a violation of intestinal motility. In the later stages of intestinal cancer, persistent abdominal pain appears, which is aching in nature without clear localization.
First signs
It is not possible to independently identify cancer before the onset of severe symptoms. This is due to the fact that the signs of pathology are nonspecific and may indicate a number of other disorders. To determine the first symptoms of intestinal cancer at an early stage, it is advisable to use instrumental methods of visualizing the walls of the organ through probing or irradiation. The doctor suspects the development of an oncological process if the patient has such first signs of early-stage intestinal cancer as:
- change in stool color to dark;
- general weakness;
- slight but persistent increase in body temperature;
- progressive weight loss;
- pallor of the skin.
Suspicions of cancer often arise when the patient complains of diarrhea or frequent constipation. In women, the formation of a tumor in the intestine may be accompanied by damage to the bladder and the occurrence of pathological communication between the rectum and vagina. This process is not accompanied by clear symptoms. In men, the appearance of a tumor in the intestines is indicated by difficulty urinating and signs of damage to the representative gland.
The main forms of colon cancer and their symptoms:
- Obstructive with the leading symptom: intestinal obstruction. With partial obstruction, symptoms manifest themselves: a feeling of fullness, rumbling, bloating, attacks of cramping pain, difficulty passing gases and feces. If the intestinal lumen decreases, acute intestinal obstruction occurs, which requires emergency surgery.
- Toxic-anemic and it leads to the development of anemia, weakness, high fatigue and pale skin.
- Dyspeptic with characteristic nausea and vomiting, belching, aversion to food, with pain in the upper abdomen accompanied by heaviness and bloating.
- Enterocolitic with intestinal disorder: constipation or diarrhea, distension, rumbling and bloating accompanied by pain, blood and mucus in the stool.
- Pseudo-inflammatory with fever and abdominal pain, minor disorders, increased ESR and leukocytosis.
- Tumor-like without any special symptoms, but during examination you can feel the tumor through the abdominal wall.
Prevention and prognosis
Early identification and prevention of the disease is possible through screening programs. We are talking about performing a stool test for the presence of occult blood, flexible sigmoidoscopy and colonoscopy. The leading measures in the framework of cancer prevention should be considered a balanced diet with the presence of products of plant origin and, accordingly, minimizing the consumption of animal fats.
When inflammatory diseases develop in the area of the large intestine, timely treatment is strongly recommended. If polyps have been identified, then it is necessary to remove them. This will improve the prognosis of the disease even despite the ICD-10 code.
Speaking directly about the prognosis, it is necessary to pay attention to the fact that if the disease is detected in the early stages, then it is favorable. For example, the five-year survival rate for the first stage of the disease ranges from 90 to 100%
At the second stage, the presented indicators range from 60 to 70% and decrease in relation to the third stage, ranging from 30 to 50%. At the last stage of the disease, the patient is not always offered treatment.
Depending on vital signs, palliative surgery is sometimes performed, after which the average life expectancy will be six to 12 months. That is why it is strongly recommended to take care of your own health and take into account all negative symptoms.
In front and above the upper part of the intestine the following organs are adjacent: the quadrate lobe of the liver, the neck and the body of the gallbladder. The hepatoduodenal ligament is located between the upper part of the intestine and the left lobe of the liver (lower surface). At the base of this ligament lies the common bile duct. The upper part of the duodenum, not covered by peritoneum, is in contact with the portal vein, common bile duct, and arteries (gastroduodenal and pancreatic-duodenal).
The posterior surface of the descending part of the intestine is in contact with the pelvis of the right kidney, ureter, and renal vessels. The hilum of the kidney is slightly covered by the duodenum. The descending part of the duodenum is in contact with: the right curvature of the colon, the ascending colon, and the head of the pancreas.
The common bile duct is often located in the parenchyma of the head of the pancreas, then it connects with the pancreatic duct and flows into the duodenum. On the surface of the intestinal mucosa there is a small longitudinal fold (up to 1 cm long), on the surface of which there is a large duodenal papilla, on which the pancreatic duct opens. Sometimes there is an accessory pancreatic duct that opens higher than the main one.
Between the descending part of the duodenum and the head of the pancreas, a groove is formed in which the common bile duct lies. The superior mesenteric vein and artery are adjacent to the lower part of the duodenum. These vessels are located at the root of the mesentery. Further along this section the transverse colon and loops of the small intestine are adjacent.
Sometimes the duodenum can be compressed by the superior mesenteric arteries, leading to obstruction. In the clinic, such cases are called arterio-mesenteric obstruction, which often occurs with prolapse of the small intestine and some other organ diseases. Retroperitoneal tissue and loops of the small intestine surround the ascending part of the duodenum. The lower part of the intestine crosses the aorta at different levels: above or below the bifurcation.
The intestinal walls are constructed as follows:
- serous membrane;
- muscle layer;
- mucous membrane.
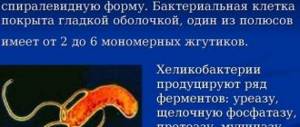
Between the mucosa and the muscle layer is the submucosa. The mucous membrane is covered with many villi. The villi are lined with prismatic bordered epithelium, which significantly increases the absorption capacity of this part of the gastrointestinal tract. Between these epithelial cells are goblet enterocytes that produce glycoproteins and glycosaminoglycans. The hormones enteroglucagon, gastrin and secretin are produced by other cells - Paneth or intestinal enterocytes. The duodenal bulb has longitudinal folds, the rest of the small intestine has circular folds. Due to the common bile and pancreatic ducts, a longitudinal fold of the mucous membrane is formed.
The mucosa contains lymphatic follicles, lymphocytes and plasma cells. The submucosa contains duodenal or Brunner's glands, the ducts of which open on the surface of the intestinal crypts.
The muscular layer of the intestine consists of non-striated muscle fibers arranged in two layers. The outer layer is longitudinal, the inner layer is circular. Serosa covers the duodenum partially, for a short distance. The remaining parts of the intestine are covered with adventitia, which is loose connective tissue. Numerous vessels and nerves pass through it.
Which environment predominates in the lumen of the duodenum depends on the stage of digestion. Before digestion begins, the environment is slightly alkaline (pH from 7.2 to 8.0). When the acidic contents of the stomach enter the intestine, the reaction changes towards acidic, but is then quickly neutralized and restored to its previous levels. The acidic environment is neutralized by pancreatic juice and other digestive juices.
Causes of Payr's syndrome
Pain and discomfort in the gastrointestinal tract have many different causes, pain in the splenic angle is no different. Here are a number of reasons: 1. Pronounced bending of the colon in the splenic angle. May be a consequence of coloptosis (low position of the transverse colon). Coloptosis can be either a congenital anomaly (for example, a long transverse colon) or observed in overweight patients. In general, coloptosis is often observed in obese people. Why is the large intestine also called Intestinum Crassum in honor of the commander Marcus Licinius Crassus (who suppressed the uprising of Spartacus), a very plump man.
The long transverse colon results in the formation of a very strong bend at the splenic angle
2. Accumulation of gases. This is believed to be the most common cause of splenic flexure syndrome and is due to excess gases in the large intestine. In order for the patient to get rid of discomfort, it is necessary to reduce gas formation and improve the release of gases. 2. Bloating. Here there is more due to neighboring organs, for example, the stomach. Excessive gas production can be caused by poor digestion of food in the stomach and small intestine. Or due to the so-called aerophagia - swallowing air. This is a fairly common cause of colic in newborns (aerophagia when screaming and crying). This can occur when drinking quickly, chewing gum, or breathing through the mouth. 3. Inflammatory bowel diseases (nonspecific ulcerative colitis and Crohn's disease). With these diseases, the intestinal mucosa suffers quite severely. 4. Food poisoning. Most often caused by various bacterial agents (salmonella, staphylococcus, clostridia, pathogenic strains of E. coli). 5. Postoperative period. Against the background of postoperative paresis (functional weakening of peristalsis). This can lead to pain in the left hypochondrium. 6. Various obstacles. This is usually cancer of the descending colon. 7. Functional weakening of peristalsis during peritonitis. 8. Intestinal obstruction. 9. Changing the composition of the diet. The presence of a large amount of short-chain carbohydrates in the diet: they can retain water in the intestinal lumen and enhance fermentation processes. Examples: apples, prunes, Brussels sprouts, cherries. Products that increase flatulence: potatoes, soybeans, peas, broccoli, alcohol.
Possible complications and consequences
Any surgical intervention is dangerous due to its complications, and such cancer therapy is no exception. The first sign of the development of postoperative complications is blood leaks into the abdominal cavity.
In the early period after surgical therapy, poor wound healing and damage by bacterial microflora may be observed. All this worsens the patient's condition. When such complications occur, the consequences can be very unfavorable. A weakened body may not be able to cope with the additional load, which can cause blood poisoning and death.
The list of dangerous complications of surgery and consequences that can lead to death after intestinal intervention includes insufficient anastomosis. This term hides the unsatisfactory fastening of two segments as a result of eliminating the affected area. If sutures are placed incorrectly, the joint may become thin and tear. In this case, the contents of the intestine are poured into the abdominal cavity, provoking the development of peritonitis - an extremely dangerous condition that often causes the death of the patient.
A common complication after surgery is digestive disorders. Many patients complain of the development of flatulence and defecation disorders that occur after eating. This leads to the fact that patients have to completely change their taste preferences, giving preference to monotonous food that does not cause such effects and is well tolerated by the body.
After surgery, adhesive disease may develop. In this case, fibrous tissue seems to glue the intestines and abdominal organs together. This disorder can cause poor intestinal obstruction and provoke pain and defecation disorders. The adhesive process poses a danger not only to the health, but also to the life of the patient and often requires additional surgical interventions.
Symptoms of colon pathology
You can suspect that there are problems with the colon based on the following symptoms:
- Pain. They can be aching and spasmodic. Localization of unpleasant sensations is the left and right lower abdomen, the area above and below the navel. Spasms and soreness force the patient to go to the toilet, since the act of defecation brings relief. There is usually no connection between food and the appearance of pain, with the exception of inflammatory processes in the transverse colon, which is located under the stomach and reacts with reflex contractions to its excessive filling.
- Chronic constipation. There are rare stools (less than 3 times a week), difficult bowel movements, and a feeling of incomplete bowel movement.
- Diarrhea. It bothers you constantly, or appears sporadically, alternating with constipation.
- Bloating. Occurs after eating food that does not usually cause this symptom.
- Flatulence is excessive accumulation and release of gases in the intestines.
- Streaks of blood and mucus in the stool.
Clinical picture and diagnosis
Adenocarcinoma of the colon and rectum grows slowly, and it takes a long time before it becomes large enough to cause symptoms
For early diagnosis, it is important to carry out routine examinations regularly. The symptoms that develop depend on the location, type and extent of the lesion, as well as complications
The ascending colon has a large lumen, a thin wall and liquid contents, so obstruction occurs only in the later stages; carcinomas are usually fungiform. The tumors reach large sizes and are then even palpable through the abdominal wall. Bleeding is usually hidden. Complaints may be limited to fatigue and weakness due to severe anemia.
The lumen of the descending colon is smaller, the feces are semi-solid, and the cancer tends to surround the colon circumferentially, causing alternately constipation and frequent bowel movements. The clinical picture can be represented by symptoms of partial obstruction with colicky abdominal pain or complete obstruction. There may be blood in the stool, streaked or mixed with stool.
With colorectal cancer, the most common symptom is bleeding during bowel movements. In any case of rectal bleeding, even with obvious hemorrhoids or diverticular disease, the possibility of concomitant cancer should be considered. There is tenesmus or a feeling of incomplete bowel movement. It is characteristic that there is no pain until the perirectal tissue is affected.
Simple fecal occult blood testing is recommended as part of population screening and surveillance programs in cases of high risk of colorectal cancer. If the test results are positive, further research is required. For greater data reliability, the patient should follow a high-fiber diet without meat products for 3 days before the analysis.
In approximately 65% of cases, colorectal cancer is localized within the reach of fibrosigmoscopy. If cancer is suspected in any part of the large intestine, in all cases of symptoms that may be associated with the colon, fibrocolonoscopy is needed. If a lesion is detected by sigmoidoscopy, a total colonoscopy is performed and the lesions found in the colon are completely removed. Endoscopic excision of existing polyps can reduce the total length of the section of intestine that must be removed. Fractional endoscopic biopsy of polyps is misleading in 25% of cases, and its negative result does not completely exclude cancerous degeneration of the polyp. If the tumor has a wide base or cannot be removed endoscopically, surgical excision is resorted to.
X-ray with barium enema is unreliable for detecting rectal cancer, but is important as a first step in diagnosing colon cancer. When examining with air contrast, smaller lesions (less than 6 mm) are visible than when using a barium enema with filling the lumen, but air in the colon (pneumocolon) in 20-30% of cases prevents the detection of large lesions (more than 2 cm)
Before examining the colon with barium or by endoscopy, it is important to prepare the bowel well, which often requires laxatives, oral irrigation, and repeated enemas. If a lesion obstructing the colon lumen is suspected, barium should not be given orally because absorption of water from the barium suspension in the colon may precipitate barium sulfate and cause complete obstruction of the colon.
Even if X-ray diagnosis is quite reliable, a colonoscopy should be done; 30% of tumors and 40% of polyps are not detected during barium enema examination, and colonoscopy allows the identification of simultaneously present lesions, which determine the total length of the part of the intestine to be resected.
An increase in the content of carcinoembryonic antigen in the blood serum is not specifically associated with colorectal cancer, but in 70% of patients its level is high. If this indicator is high before surgery, and becomes low after removal of the colon tumor, monitoring it will help determine relapse. The levels of other tumor markers CA 19-9 and CA 125 may also be elevated.
Diagnosis, treatment and prognosis for colon cancer. How to prepare for surgery?
Diagnosis of colon cancer (as well as the entire intestine) is carried out using:
- Physical examination, during which the patient’s condition is assessed: the color of the skin, the presence of fluid in the peritoneal cavity (determined by tapping). It is possible to determine the approximate size of the tumor through the abdominal wall only with large nodes.
- Laboratory blood tests, including determination of specific antigens, stool for the presence of blood.
- Instrumental research methods: sigmoidoscopy to assess the condition of the lower intestine, colonoscopy to examine and obtain tissue for biopsy, X-ray with a barium suspension to identify the location of the tumor, ultrasound and CT to clarify the extent of the oncological process and a clear image of the anatomical structures.
Sigmoidoscopy
Treatment of colon cancer
Treatment of colon (bowel) cancer is carried out by radical surgery followed by radiation and chemotherapy. The doctor takes into account the type and location of the tumor, the stage of the process, metastases and concomitant diseases, the general condition of the patient and age.
Treatment of colon cancer without complications (obstruction or perforation) and metastases is carried out by radical surgery with removal of the affected areas of the colon with the mesentery and regional lymph nodes.
If there is a tumor in the colon on the right, a right-sided hemicolonectomy is performed: the cecum, ascending colon, a third of the transverse colon and 10 cm of the ileum in the terminal section are removed. Regional lymph nodes are simultaneously removed, and an anastomosis is formed (connection of the small and large intestines).
If the colon is affected on the left, a left-sided hemicolonectomy is performed. An anastomosis is performed and the following is removed:
- one third of the transverse colon;
- descending colon;
- part of the sigmoid colon;
- mesentery;
- regional LU.
A small tumor in the center of the transverse section is removed, as is the omentum and lymph nodes. The tumor at the bottom of the sigmoid colon and in its center is removed from the lymph nodes and mesentery, and the large intestine is connected to the small intestine.
If the tumor spreads to other organs and tissues, the affected areas are removed using a combined operation. Palliative operations are started if the form of cancer has become inoperable or advanced.
During the operation, bypass anastomoses are applied to the sections of the intestine between which there is a fecal fistula in order to exclude acute intestinal obstruction. To completely shut off, the afferent and efferent loops of the intestine are sutured between the anastomosis and the fistula, and then the fistula along with the turned off part of the intestine is removed. This operation is relevant in the presence of multiple fistulas and high fistulas with a rapid deterioration of the patient’s condition.
Informative video: treatment of colon cancer with surgery
How to prepare for surgery
Before the operation, the patient is transferred to a slag-free diet and is prescribed cleansing enemas and castor oil 2 days before. Potato dishes, any vegetables, and bread are excluded from the diet. For preventive purposes, the patient is prescribed antibiotics and sulfonamides.
Read here: Skin cancer on the back
Immediately before the operation, the intestines are cleansed using the laxative Fortrans or orthograde lavage of the intestines is performed using an isotonic solution administered through a tube.
Radiation and chemotherapy
Radiation therapy in the tumor growth area begins 2-3 weeks after surgery. In this case, side symptoms are often observed due to damage to the mucous membrane in the intestines, which are manifested by lack of appetite, nausea and vomiting.
The next stage is chemotherapy with modern drugs to eliminate side effects. Not everyone can easily tolerate chemotherapy, so in addition to nausea and vomiting, allergic skin rashes and leukopenia (a decrease in the concentration of leukocytes in the blood) may occur.
Postoperative measures
During the first 24 hours, the patient does not eat and receives medical procedures to eliminate shock, intoxication and dehydration. On the second day, the patient can drink and eat semi-liquid and soft food. The diet is gradually expanding:
- broths;
- mashed porridge;
- vegetable purees;
- omelettes;
- herbal teas;
- juices and compotes.
Important. To avoid constipation and the formation of a fecal lump, the patient should take petroleum jelly twice a day as a laxative. This measure prevents injury to fresh sutures after surgery.
Stages
In intestinal cancer, the stages of the pathological process are determined based on several parameters, including the intensity of growth of the primary tumor, the severity of symptoms and the presence of metastases to distant organs. In medical practice, the most often used classification takes into account 4 stages of the oncological process. Some clinicians also distinguish stage 0, which is characterized by the presence of a cluster of cells that have an atypical structure and the ability to rapidly divide.
At stage 1 of the pathological process, malignant degeneration of the existing tumor begins, which is accompanied by its rapid increase in size. The formation has not yet left the wall of the affected area of the intestine. Metastases to regional lymph nodes and no pain are observed. During this period of cancer development, patients may periodically show signs of mild eating disorders. A colonoscopy at this stage of tumor formation makes it possible to identify it.
At stage 2, the malignant formation reaches a size of 2–5 cm. It grows to the entire depth of the intestinal wall. There are still no signs of the onset of tumor metastasis. The severity of disorders of the digestive system is aggravated. Any instrumental research methods can identify a neoplasm.
At stage 3 of the oncological process, there is an increase in the activity of cells with an atypical structure. This leads to a rapid increase in the size of the existing tumor. It begins to spread beyond the intestines, affecting nearby lymph nodes and internal organs. Symptoms of damage to the gastrointestinal tract become pronounced.
Stage 4 of intestinal cancer is considered the most dangerous. It is characterized by rapid growth of tumor tissue and metastasis to distant organs. The severity of symptomatic manifestations of the pathological process becomes critical. In addition, the human body is poisoned by toxic substances released by the tumor. Disruptions in the functioning of all body systems are increasing.
Diseases of the sigmoid colon
Diseases of this section of the digestive system become a consequence of fecal obstruction, arising due to a violation of the elasticity of the walls of the sigmoid intestine, with the detrimental effect of intoxication products on the gastrointestinal tract. All diseases of the sigmoid colon are accompanied not only by an internal inflammatory process and an acute attack of pain, but also by external changes in this section and its epithelial layer. Such changes can be tracked clinically - using ultrasound. Early diagnosis helps avoid serious complications in the future.
Dolichosigma intestinalis
Even a child can be diagnosed; it is important to treat the disease in a timely manner. Dolichosigma is a pathological elongation of the sigmoid colon or mesentery (mesocolon), as a result of which intestinal motility is disrupted. In such a clinical picture, megadolichosigma is observed, i.e. abnormal thickening of the walls. Constipation and paroxysmal abdominal pain are eloquent signs of the disease, but in order to determine the fact of damage to the large intestine, a comprehensive diagnosis is required.
Cancer
Adenocarcinoma, neoplasia carcinoma, blastoma, distal tumor are malignant neoplasms that, with successful treatment, reduce the quality and life expectancy. For example, a villous tumor of the sigmoid colon is difficult to diagnose at an early stage; the symptoms are similar to classic food poisoning (bloating, flatulence, diarrhea, nausea). The approach to the problem is comprehensive and includes diagnostics of the body with biopsy and sigmoidoscopy. Treatment is carried out surgically - removal of the tumor with long-term rehabilitation.
Inflammation
If an inflammatory process occurs in the sigmoid part of the intestine, in medical practice this disease is called sigmoiditis, and is treated with conservative methods. Common causes of the disease are increased activity of intestinal infections and an imbalance of bacteria (dysbacteriosis). Doctors remind us of radiation sickness and intestinal ischemia, pressure of neighboring organs and impaired circulation as pathogenic factors that can provoke the first attack.
With progressive inflammation, doctors recommend taking painkillers and additionally drinking probiotics to restore intestinal microflora. To destroy pathogenic flora, treatment of sigmoiditis necessarily includes the prescription of antibiotics. Vitamin therapy and a therapeutic diet also become an integral part of an integrated approach to health problems. It all depends on the form of the characteristic disease. It could be:
- proctosigmoiditis (spastic colitis);
- focal sigmoiditis;
- bend;
- erosive sigmoiditis.
Diverticulosis
If the blood supply to tissues is impaired and improper transportation of feces to the intestines, the patient develops another disease. It is called diverticulosis and is relapsing in nature. The inflammatory process spreads to the sigmo-rectal sphincter, which connects the rectum and sigmoid colon and is responsible for the excretion of feces.
The disease starts with an acute attack of pain, which is localized in the left side of the abdomen. During the pathological process, intestinal motility is impaired, and high intraluminal pressure occurs. The patient cannot understand its cause for a long time, and the truth is revealed by ultrasound. Inflammation of diverticula of the sigmoid colon is treated conservatively in a hospital setting.
Find out in more detail what sigmoid colon diverticulosis is - symptoms and treatment of the disease.
Colon cancer
Colon cancer is a malignant tumor that grows from the mucosa. The risk group includes older people, and it occurs more often in men, and the likelihood of occurrence in adolescents is practically absent.
The disease is fatal. However, it cannot be said that colon cancer is incurable - there is always a chance to survive. Timely detection and qualified medical care make it possible to save a person’s life. Its duration and prognosis depend on the histological structure of the tumor.
The urgency of the problem lies in the fact that colon cancer develops asymptomatically for a long time, or people attribute its symptoms to another disease. This approach is dangerous, since it makes sense to seek treatment while the cancer is curable and its consequences are reversible. If left untreated, death occurs.
The incidence of colon cancer is 2.5–5%, and the mortality rate is increasing every year. Epidemiology and statistics show that it is higher in economically developed countries. Every year, about 800 thousand cases of illness are detected in the world, of which 15 thousand are in Russia.
Types of Colon Cancer
The location, size and types of tumor formation play a role in the choice of treatment method.
Based on the location of the primary focus, the following types of colon cancer are distinguished:
- • ascending department,
- • descending,
- • transverse colon,
- • bending of the splenic or hepatic angle.
Complicated forms occur when the cancer spreads to the cecum or sigmoid colon. Growth can be directed both into the intestinal lumen and along the walls.
Based on the cytological picture, the following types are distinguished:
- • adenocarcinoma,
- • signet ring cell carcinoma,
- • mucinous adenocarcinoma,
- • squamous cell,
- • glandular-squamous,
- • undifferentiated.
There is also an international TNM classification, which takes into account the size, distribution, metastases, and the presence of proliferation in the lymph nodes.
Colon cancer, symptoms and signs with photos
The onset of colon cancer is difficult to detect and there are no visible changes on the body (eg, skin spots, ulcerations). Symptoms resemble other diseases of the gastrointestinal tract (cholecystitis, appendicitis), and patients complain of dyspeptic symptoms - nausea, bloating, stool disorders. Pain syndrome appears later, when the tumor grows into surrounding organs.
Primary external manifestations at an early stage are not pronounced; colon cancer is usually asymptomatic. Precursors of cancer that can cause its development are chronic colitis and polyposis. However, the patient may not notice the very initial,
Divisions, types and forms of colon cancer. Localization of tumors
What does the large intestine consist of?
Clinically, colon cancer manifests itself depending on the location of the tumor in its parts, the degree of spread and complications that aggravate the course of the primary cancer.
If cancer of the ascending colon , symptoms manifest as pain in 80% of patients more often than with a tumor of the descending colon on the left. The cause is a violation of motor function: pendulum-like movement of contents from the small intestine to the cecum and back. The tumor can be palpated through the abdominal wall, which indicates cancer of the ascending colon; the prognosis will depend on the stage, the presence of metastases, successful treatment, restoration of motor (motor-evacuation) function, and the absence of intoxication of the body.
Transverse colon cancer with spastic contractions of the intestine, which push feces through a narrow lumen near the tumor, causes sharp pain. They are aggravated by the perifocal and intratumoral inflammatory process of the intestinal wall, accompanied by infection from disintegrating tumors.
Transverse colon cancer initially does not manifest itself as pain syndromes until the tumor spreads beyond the intestinal wall, moving to the peritoneum and surrounding organs. Then the tumor can be palpated through the anterior wall of the peritoneum, and pain will occur with varying frequency and intensity.
Cancer of the hepatic flexure of the colon leads to narrowing and obstruction of the intestinal lumen. Sometimes the surgeon is unable to insert an endoscope there due to deep infiltration of the mucous membrane and stiffness.
Cancer of the hepatic angle of the colon may take the form of a disintegrating tumor in the hepatic flexure of the colon, which grows into a loop of the duodenum. With such dislocation of the tumor, chronic diseases are stimulated: gastric and duodenal ulcers, adnexitis, cholecystitis and appendicitis.
There is a threat of intestinal obstruction, a colonic fistula or in the duodenum is possible. Cancer of the ascending colon , like the hepatic angle, can also be complicated by subcompensated stenosis of the duodenum and impaired colonic patency, atherosclerotic cardiosclerosis and secondary hypochromic anemia.
With this diagnosis, a right-sided hemicolectomy and gastropancreatoduodenal and resection of perirenal fat on the right side, excision of metastasis from the liver if it is present in the 7th segment of the organ, are required.
Cancer of the splenic flexure of the colon , descending colon and sigmoid colon occurs in 5-10% of patients with intestinal cancer. The pain syndrome can be combined with a hyperthermic reaction (increase in temperature), leukocytosis and rigidity (tension) of the abdominal wall muscles in the front and left. Feces can accumulate above the tumor, which leads to increased rotting and fermentation processes, bloating and retention of stool and gases, nausea, and vomiting. At the same time, the normal composition of the intestinal flora changes, and pathological discharge from the rectum appears.
Read here: Pancreatic Oncology
Stages of cancer development and prognosis
Bowel cancer develops in four stages.
| Stage | Colon cancer | Rectal cancer |
| First | The neoplasm is of modest size, located deep in the intestinal mucosa. Metastases to the lymph nodes are not detected. | The cancerous tumor is moving, the size does not exceed 2 cm. There are no metastases or ingrowth into the intestinal wall. |
| Second | The tumor is enlarged, but does not leave the border of the intestine; single metastases to the lymph nodes are possible. | The first option: the tumor covers about 50% of the diameter of the intestine, there are no secondary foci of cancer, but possible growth into muscle tissue. Second: the size is similar to the first type, there are metastases in regional lymph nodes. |
| Third | The tumor covers most of the diameter of the intestine, is distributed throughout the entire wall, and the presence of multiple secondary foci is possible. | The neoplasm grows into the walls surrounding tissues and organs. Numerous metastases are possible. The tumor size is more than 50% of the intestinal semicircle. |
| Fourth | A neoplasm of impressive size, growing into nearby organs, with multiple secondary foci in the lymph nodes. | A large, immobile tumor that spreads to neighboring organs and tissues in the pelvic cavity, with numerous metastases, or is mobile in distant secondary foci. |
The international classification of stages of cancer tumor development is the TNM system. A brief and accurate guide to describing cancer, allowing you to obtain undistorted information. The first component T is the primary tumor, the second N is lymph nodes, the third M is distant metastases. The numbers next to the letter indicate the degree of development of the disease.
| T – tumor | N – lymph nodes | M – metastases | |||
| T0 | Undiagnosed primary tumor. | N0 | There are no secondary lesions in regional lymph nodes. | M0 | There are no distant metastases. |
| T1 | The tumor occupies less than half the diameter of the intestinal walls and does not grow into muscle tissue. | N1 | Expanding the extent of damage to regional lymph node metastases. Damage to 1-3 lymph nodes. | M1- 4 | Distant metastases present, their number |
| T2 | The neoplasm occupies more than half the diameter of the intestinal walls and grows into the muscle layer. | N2 | There are metastases in more than 4 regional lymph nodes. | ||
| T3 | Cancer affects all layers of the intestinal wall, and there is a risk of intestinal obstruction due to a narrowed lumen in the intestine. | NX | There is insufficient data to assess the extent of regional lymph node involvement. | ||
| T4 | The tumor grows into neighboring organs. Persistent, complete narrowing of the lumen in the intestine. | ||||
| TX | The primary tumor cannot be assessed due to lack of sufficient data. | ||||
| Tis | Carcinoma in the initial stages of development. |
The question of how long people live with this pathology and after its treatment does not have an exact answer. Life expectancy depends on the stage of cancer at which treatment began, at what age the disease began, whether the patient has other pathologies, etc.
Five-year survival rate after radical surgical treatment is 45-50%.
If treatment began at the first, second stage the prognosis is much better and will be 85-95% survival. At the third stage, cancer is curable by 65-70%. The most dangerous fourth stage leaves a 35% chance of overcoming the disease.
Diseases
Where is the colon located and how does it hurt? First of all, a person who has inflammation of this part of the organ will feel pain in the lower abdomen and discomfort in the anus .
In addition, other signs of pathology may be observed:
- regular constipation;
- discharge of pus from the anus;
- the presence of blood impurities in the stool;
- flatulence;
- painful urge to defecate;
- loose stool.
If a person has pain in the upper, transverse, descending colon, symptoms of pathology may also indicate iron deficiency anemia . This occurs due to the formation of bleeding ulcers or erosions in the affected organ.
Diseases of the colon occur for the following reasons:
- lifestyle errors: physical inactivity, overeating, abuse of fatty foods;
- hypotension;
- chronic constipation;
- abuse of dietary supplements of dubious quality;
- long-term treatment with antibiotics.
The colon, the symptoms of inflammation of which cannot be ignored, is susceptible to many diseases, including the formation of a malignant tumor .
Hirschsprung's disease
This is a hereditary pathology that manifests itself in a person in infancy or early childhood..
A person with this disease suffers from prolonged constipation, which can last over several weeks.
In this case, enemas and laxatives are useless. However, constipation in Hirschsprung's disease alternates with debilitating diarrhea.
All these disorders of the functioning of the digestive system occur due to ganglion cells of the colon.
The parts of the intestine located above it hypertrophy due to constant contractions , which is why the intestines cease to empty themselves. With this disease, a person is indicated for surgery to remove hypertrophied parts of the organ.
Untimely treatment of the pathology can lead to such serious consequences as intestinal perforation, internal bleeding and even peritonitis.
Diverticulosis
The disease can be either congenital or acquired. Diverticulosis is a disease that is accompanied by protrusion of sections of the intestinal mucosa through its muscular layer . This is accompanied by the formation of sac-like formations in which feces can accumulate, which can provoke inflammation of the organ mucosa.
Typical symptoms of diverticulosis include lower abdominal pain, nausea, diarrhea and vomiting . Ignoring treatment for diverticulosis can lead to such serious consequences as organ obstruction, phlegmon and peritonitis.
Read this article about what diverticula are and how they are treated.
Polyposis
A disease accompanied by the formation of growths on the mucous membrane of the organ , the size of which ranges from a few millimeters to several centimeters.
Polyps are dangerous because they can degenerate into malignant neoplasms, that is, provoke intestinal cancer.
Symptoms of the disease include problems with defecation, since growths in the lumen of the organ interfere with the free movement and exit of feces.
If the polyps are large, the patient may suffer from hemorrhages inside the organ. Polyposis is treated surgically, as well as using cytostatic drugs.
Oncology
Often, inflammation of the colon, the symptoms and treatment of which is extremely important, leads to cancer of this part of the intestine. Oncologists consider colon cancer the least dangerous type of cancer of the gastrointestinal tract . However, the threat of this disease to human life lies in the fact that the symptoms of the disease resemble signs of a disorder in the functioning of the gastrointestinal tract.
So, the patient suffers from symptoms such as diarrhea, pain and colic in the lower abdomen, slight discharge of blood and mucus during bowel movements. But as the disease progresses, symptoms such as anemia and prolonged constipation, caused by a narrowing of the lumen of the colon, increase.
In this case, cancer is treated surgically: the affected part of the organ is removed along with part of the mesentery and nearby lymph nodes.
If metastases occur after surgery, a course of chemotherapy is given.
In the first stages of the disease, the prognosis for patient survival is 70%, but in the last stages of cancer the probability of death is at least 80% .
Possible symptoms of colon cancer cannot be ignored, because timely consultation with a doctor will allow treatment of the disease to begin as early as possible.
Features of digestion and organ functions
From the stomach, food in a liquid or semi-liquid state enters the duodenum. The pyloric part of the stomach performs peristaltic contractions and pushes the bolus of food towards the sphincter. The latter's receptors send a signal along the vagus nerve, and the sphincter opens. The opposite happens when the food bolus irritates the organ's receptors. The muscle sphincter remains closed until the chyme moves further through the intestines. The main functions of the duodenum: participation in the process of digestion and absorption of nutrients. The next stage of digestion begins in this section of the intestine. The common bile and pancreatic ducts open on the surface of the nipple of Vater. The process of digestion of food is carried out by pancreatic juice, intestinal juice and bile. All these components have a pronounced alkaline reaction, so the acidic environment of food coming from the stomach is quickly neutralized. Pancreatic juice contains organic and inorganic substances. The first include proteolytic, lipolytic, aminolytic enzymes. Proteins are broken down by trypsin, chymotrypsin, elastase and carboxypetidase. Inhibitors of proteolytic enzymes protect the pancreas from self-digestion. Lactase, maltase and amylase break down carbohydrates into monosaccharides. Phospholipase and lipase break down fats into simpler components (glycerol and fatty acids). Liver cells secrete bile into the intestinal lumen. Externally, it is a liquid with an alkaline reaction, golden yellow. Dry residue contains up to 2.5%. Main components: pigments, bile acids, cholesterol. From 0.5 to 1.2 liters are produced per day. This process is continuous, however, bile enters the intestines only during meals. The rest of the time, bile is in the gallbladder. Bile is necessary to activate pancreatic enzymes. In particular, lipases. Emulsification of neutral fats is carried out by fatty acids. In addition, bile enhances the peristalsis of the intestinal walls, increases the production of pancreatic juice, and acts as a bacteriostatic substance, preventing the development of putrefactive bacteria.
Bowel cancer treatment
The leading treatment for bowel cancer is surgery, in which the surgeon removes both the tumor itself and nearby lymph nodes (to prevent the cancer from spreading).
In some cases, small tumors are removed using a sigmoidoscope (a long flexible tube inserted through the anus into the rectum). However, more often a more extensive intervention is required, in which the anterior abdominal wall is dissected. Sometimes, after removing the affected part of the intestine, the surgeon connects the resulting ends with each other. If connection is not possible, removal of the intestine to the anterior abdominal wall is indicated. Most often, this is only the first stage of the operation, and in the future, to restore the normal path of waste of feces, the ends of the intestine are connected. However, in ten percent of cases the patient still has to live with the colon removed.
In some cases, a course of chemotherapy or radiation therapy is performed to destroy any cancer cells that may remain after surgery.
Typically, a course of radiation therapy lasts four to six weeks. This type of therapy is completely painless, but can cause various side effects, which gradually disappear after stopping treatment. Side effects of radiation therapy: fatigue, loss of appetite, nausea, vomiting, hair loss, minor subcutaneous hemorrhages, itching or redness of the skin. In women, the following manifestations may be added: vaginal dryness, hot flashes, as well as other symptoms characteristic of menopause.
Drug therapy (chemotherapy) is given in cycles lasting from several weeks to months. Medicines are prescribed both in injections and in tablets. Most people continue to work during this treatment, despite the presence of such side effects as: constipation or diarrhea, loss of appetite, nausea, vomiting, decreased resistance to infections, formation of mouth ulcers, decreased attention, decreased libido, loss of hair. . In women, drug therapy causes the same specific effects as radiation therapy.
If the cancer has not spread beyond the colon, the five-year survival rate is about 99%. When a tumor grows into the intestinal wall, the five-year survival rate is about 85%. When regional lymph nodes are involved, the five-year survival rate drops to 60%. If the process spreads to distant lymph nodes, the five-year survival rate is less than 30%.
Diagnosis and treatment
The absence of characteristic symptoms specific to intestinal cancer indicates the need for additional examination methods to be able to detect the disease at an early, first stage.
The specialist should pay special attention to the patient’s complaints regarding the characteristics of abdominal pain, uncontrolled weight loss, and pale skin. Based on the patient’s complaints and the following research methods, there is a chance to identify the disease as early as possible and begin treatment
- Palpation is the simplest and most mandatory method of medical examination of the large intestine, which allows one to identify the size and location of a malignant tumor. To ensure the reliability of the information, palpation is carried out in different positions of the patient’s body.
- Sigmoidoscopy and colonoscopy are types of instrumental diagnostics that make it possible to detect cancer at the first, early stage. Their participation allows us to describe in detail the location and size of the tumor, and take the affected tissue for analysis.
- Irrigoscopy is an x-ray diagnostic method carried out through an enema, the introduction of a barium suspension into the intestines.
- Ultrasound, laparoscopy, computed tomography are used to detect distant metastases.
Treatment is only surgical, necessarily supplemented with chemotherapy. Preparation for surgery is aimed at completely cleansing the intestines through enemas, taking laxatives, and following a certain diet.
The operation involves resection of the tumor and regional lymph nodes, with anastomosis to restore intestinal patency. The choice of operating method is determined by the stage of cancer development, possible complications, metastases, age and general condition of the patient.
Diagnostics
A proctologist is involved in identifying and treating pathologies of the colon. The examination plan for patients with symptoms of diseases of this organ includes:
- Colonoscopy. Endoscopic examination of the large intestine is carried out through the anus. The endoscopist examines the mucous membrane of the organ in real time and takes material from suspicious areas for histological analysis.
- Irrigoscopy. This method of X-ray diagnostics with contrast allows you to clearly visualize defects of the intestinal wall, identify neoplasms and defects of the colon.
- Histological examination. Studying the morphology of a tissue sample taken from the intestine is the most reliable way to diagnose cancer, ulcerative colitis, Crohn's and Hirschsprung's disease.
- Coprogram. Examination of stool smears under a microscope is carried out to identify signs and possible causes of the inflammatory process in the small intestine and to assess the evacuation function of the intestinal tract.
- Culture of stool for microflora. If the infectious nature of the inflammatory process is suspected, this analysis makes it possible to make an accurate diagnosis and isolate the pathogen, which is extremely important for selecting antibacterial treatment.
We recommend reading:
Intestinal inflammation: signs of pathology, use of diet and drugs for treatment