Diagnostics
Diagnostic criteria
Complaints and anamnesis: pain in the navel and pyloroduodenal area, severe dyspeptic symptoms (nausea, belching, heartburn, less often - vomiting); combination of early and late pain; loss of appetite, weakness, fatigue, headache, sleep disturbance, local hyperhidrosis.
Physical examination: signs of polyhypovitaminosis, moderate symptoms of chronic intoxication, pain in the pyloroduodenal area in the navel area.
Laboratory tests: CBC, OAM - without features, coprogram - symptoms of impaired digestion (determination of neutral fat, undigested muscle fibers), stool may be positive for occult blood. Diagnosis of H. pylori (cytological examination, ELISA - detection).
Instrumental studies: fibrogastroduodenoscopy - endoscopic changes in the mucous membrane of the stomach and duodenum (swelling, hyperemia, hemorrhage, erosion, atrophy, hypertrophy of folds, etc.).
Indications for consultation with specialists:
1. ENT.
2. Dentist.
3. Physiotherapist.
List of main diagnostic measures:
1. General blood test (Er, Hb, L, leukoformula, ESR).
2. General urine analysis.
3. Coprogram.
4. Ultrasound of the abdominal organs.
5. Esophagogastroduodenoscopy.
6. Diagnosis of H. pylori (breath test, HpSA in stool, determination of IgG to HP, urease test, brush cytology).
7. Consultation: dentist.
8. ENT.
9. Consultation: neurologist.
List of additional diagnostic measures:
1. Electrocardiography.
2. Histological examination of the biopsy specimen.
3. Daily pH-metry of the upper gastrointestinal tract - (implementation required).
4. Determination of serum Fe.
5. Determination of diastase.
6. Electroencephalography.
7. Study of gastric juice.
8. X-ray examination of the upper gastrointestinal tract with barium.
Short description
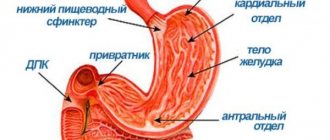
Hiatal hernias can be congenital or acquired; sliding and paraesophageal hernias are also distinguished. With a sliding hernia, the cardiac part of the stomach moves freely into the posterior mediastinum through the dilated esophageal opening of the diaphragm. Such hernias do not cause strangulation. With paraesophageal hernias, which are much less common, the cardiac part of the stomach is fixed, and its fornix or antrum, and sometimes other abdominal organs (small, large intestine, omentum) are displaced to the posterior mediastinum.
In this case, infringement of the displaced organ may occur, which is manifested by sharp pain in the chest, reminiscent of angina pectoris, sudden dysphagia or vomiting mixed with blood, and symptoms of intestinal obstruction. An X-ray examination reveals a gas bubble of the stomach in the posterior mediastinum, and a contrast examination reveals displacement of the lower third of the esophagus, absence of contrast material entering the stomach or evacuation from it. With late diagnosis, necrosis of the strangulated organ occurs with the development of mediastitis, pleural empyema, and peritonitis.
Sliding hiatal hernias are clinically manifested as refluxesophagitis, as well as cardiac sphincter insufficiency. There is practically no fundamental difference between these diseases, both from a clinical and therapeutic point of view. Insufficiency of the cardia with reflux of gastric contents into the esophagus is often secondary in nature and can be caused by scleroderma, neurological diseases (pseudobulbar palsy, diabetic neuropathy), chronic alcoholism, obesity, ascites, constipation, prolonged bed rest, stress. A number of medications contribute to the development of reflux disease of the esophagus: anticholinergic drugs, beta-adrenergic agents, glucagon, antispasmodics and coronary agents, nicotine.
READ MORE: Recovery after surgery to remove a herniated disc: how long does the rehabilitation course last, procedures and reviews
Symptoms, course. Burning and dull pain behind the sternum, xiphoid process and in the epigastrium. Patients are often diagnosed with angina pectoris for a long time and treated with coronary lytic drugs. The pain intensifies in the horizontal position of the patient, when bending the body ("symptom of lacing a shoe"). The pain is accompanied by belching and heartburn. As the disease progresses, the pain becomes almost constant and is not relieved by medications. Reflux - esophagitis can result in the development of an ulcer followed by scarring, leading to stenosis of the esophagus and the appearance of dysphagia.
ICD-10 code for erosive gastritis
The International Classification of Diseases is a normative document that ensures worldwide uniformity of methods and materials. In the Russian Federation, the healthcare system made the transition to the international classification back in 1999.
According to this systematization, recognized both in our homeland and throughout the world, ailments of the digestive organs are classified according to the following designations: K00–K93 (ICD-10 code). Erosive gastritis is listed under the code K29.0 and is diagnosed as an acute hemorrhagic form.
There are other forms of this disease, and here are the designations assigned to them:
- K29.0 (ICD-10 code) – erosive gastritis (another name is acute hemorrhagic);
- K29.1 – other acute forms of the disease;
- K29.2 – alcoholic (provoked by alcohol abuse);
- K29.3 - superficial gastritis in chronic manifestations;
- K29.4 – atrophic in chronic course;
- K29.5 – chronic course of antral and fundal gastritis;
- K29.6 – other chronic diseases of gastritis;
- K29.7 – unspecified pathology.
Erosive gastritis is listed under the code K29.0 and is diagnosed as an acute hemorrhagic form
Erosive gastritis of the stomach (ICD-10 code: K29.0) is a fairly common disease of the gastrointestinal tract, characterized by the appearance of a large number of erosions (red round formations) on the mucous membrane. This pathology most often manifests itself in an acute form and is complicated by internal bleeding.
However, chronic erosive gastritis is also diagnosed (ICD-10 code: K29.0), which can manifest itself in a sluggish form of the disease or not be accompanied by symptoms at all. This type of gastrointestinal ailment is considered the longest, considering the time spent on treatment. It is most often observed in adult patients, especially men.
Forms of gastritis:
- acute ulcerative: may occur due to injuries and burns of the stomach. Manifests itself in bloody impurities in vomit and feces;
- chronic erosive gastritis (ICD-10 code: K29.0): characterized by alternating exacerbations and remissions of the disease. Erosive neoplasms reach five to seven millimeters;
- Antral gastritis: affects the lower part of the stomach. Caused by bacteria and pathogens;
K29 Gastritis and duodenitis
GASTRITIS - inflammation of the gastric mucosa. Gastritis can occur in acute or chronic (slowly developing over several months or years) form.
The cause of gastritis is most often the bacterium Helicobacter pylori, which affects the gastric mucosa. Also, chronic gastritis can occur against the background of an inflammatory disease - Crohn's disease, characterized by inflammation of the digestive tract. Long-term use of alcohol, aspirin or NSAIDs can also lead to chronic gastritis.
One form of gastritis , known as atrophic or autoimmune gastritis, is a consequence of a pathological reaction of the immune system (antibodies are produced that destroy the tissue of the gastric mucosa).
Chronic gastritis often occurs without significant symptoms, but as a result of chronic gastritis, gradual damage to the gastric mucosa can occur, which will ultimately manifest itself in symptoms similar to those of acute gastritis. Symptoms of acute and chronic gastritis are:
- pain or feeling of comfort in the stomach, often after eating;
- nausea and vomiting;
- loss of appetite;
- stomach bleeding (may not appear until anemia develops); In case of severe bleeding due to gastritis , vomiting of blood or dark, tar-like stools may be observed.
Atrophic gastritis often occurs without pain, and the only symptom of atrophic gastritis may be pernicious anemia, leading to a deficiency of vitamin B12 in the body. In atrophic gastritis, the stomach is unable to produce enough intrinsic factor, a protein necessary for the absorption of vitamin B12. Patients suffering from atrophic gastritis have an increased risk of developing stomach cancer.
Gastritis usually resolves with lifestyle changes, for example, by reducing the amount of alcohol consumed. If chronic gastritis is caused by Helicobacter pylori infection, complete recovery usually occurs after taking a course of antibiotics and antiulcer drugs.
DUODENITIS - inflammation of the duodenum.
MINISTRY OF HEALTH AND SOCIAL DEVELOPMENT OF THE RF
ORDER No. 248 November 22, 2004 “On approval of the standard of medical care for patients with chronic gastritis, duodenitis, dyspepsia” In accordance with clause 5.2.11. Regulations on the Ministry of Health and Social Development of the Russian Federation, approved by Decree of the Government of the Russian Federation of June 30, 2004 N 321 (Collected Legislation of the Russian Federation, 2004, N 28, Art. 2898), art. 38 Fundamentals of the legislation of the Russian Federation on the protection of the health of citizens dated July 22, 1993 N 5487-1 (Gazette of the Congress of People's Deputies of the Russian Federation and the Supreme Council of the Russian Federation, 1993, N 33, Art. 1318; Collection of acts of the President of the Russian Federation and the Government of the Russian Federation , 1993, No. 52, Article 5086; Collection of Legislation of the Russian Federation, 1998, No. 10, Article 1143; 1999, No. 51, Article 6289; 2000, No. 49, Article 4740; 2003, No. 2, Article 167 ; N 9, Art. 805; N 27 (part 1), Art. 2700; 2004, N 27, Art. 2711)
I order: 1. To approve the standard of medical care for patients with chronic gastritis, duodenitis, and dyspepsia (Appendix). 2. Recommend to the heads of medical organizations to use the standard of medical care for patients with chronic gastritis, duodenitis, dyspepsia” when providing medical care.
Deputy Minister V.I. Starodubov
Appendix to the order of the Ministry of Health and Social Development of the Russian Federation dated November 22, 2004 N 248
Standard of medical care for patients with chronic gastritis, duodenitis, dyspepsia
1. Patient model
1.1. Diagnostics 1.2. Treatment based on 14 days Age category: adults, children Nosological form: chronic gastritis, duodenitis, dyspepsia ICD-10 code: K29.4, K29.5, K30 Phase: exacerbation Complication: without complications Condition of provision: outpatient care
| Code | Name | Delivery frequency | Average quantity |
| A01.16.001 | Collection of anamnesis and complaints for diseases of the esophagus, stomach, duodenum | 1 | 1 |
| A01.16.002 | Visual examination for diseases of the esophagus, stomach, duodenum | 1 | 1 |
| A01.16.003 | Palpation for diseases of the esophagus, stomach, duodenum | 1 | 1 |
| A01.16.004 | Percussion for diseases of the esophagus, stomach, duodenum | 1 | 1 |
| А01.16.005 | Auscultation for diseases of the esophagus, stomach, duodenum | 1 | 1 |
| A02.12.001 | Heart rate measurement | 1 | 1 |
| A02.12.002 | Blood pressure measurement | 1 | 1 |
| A03.16.001 | Esophagogastroduodenoscopy | 1 | 1 |
| A08.05.003 | Red blood cell level test | 1 | 1 |
| A08.05.004 | Study of the level of leukocytes in the blood | 1 | 1 |
| A08.05.006 | Leukocyte ratio in blood (blood count) | 1 | 1 |
| A08.05.009 | Determination of color index | 1 | 1 |
| A08.16.004 | Examination of stomach material for the presence of helicobacteriosis | 1 | 1 |
| A08.06.002 | Morphological study of a preparation of stomach tissue | 0,1 | 1 |
| A08.06.003 | Morphological study of duodenal tissue specimen | 0,1 | 1 |
| A09.05.003 | Study of the level of total hemoglobin in the blood | 1 | 1 |
| A09.19.002 | Examination of feces for occult blood | 0,05 | 1 |
| А12.05.001 | Erythrocyte sedimentation test | 0,01 | 1 |
| А06.16.002 | X-ray of the stomach and duodenum | 0,4 | 1 |
| A09.16.004 | Intragastric determination of the concentration of hydrogen ions in gastric contents (pH) | 0,5 | 1 |
| A04.14.002 | Ultrasound examination of the gallbladder | 0,8 | 1 |
| А04.15.001 | Ultrasound examination of the pancreas | 0,8 | 1 |
| A11.16.002 | Gastric biopsy using endoscopy | 0,1 | 1 |
| A11.16.003 | Duodenal biopsy using endoscopy | 0,1 | 1 |
1.2. Treatment based on 14 days
| Code | Name | Delivery frequency | Average quantity |
| A01.16.001 | Collection of anamnesis and complaints for diseases of the esophagus, stomach, duodenum | 1 | 1 |
| A01.16.002 | Visual examination for diseases of the esophagus, stomach, duodenum | 1 | 1 |
| A01.16.003 | Palpation for diseases of the esophagus, stomach, duodenum | 1 | 1 |
| A25.16.001 | Prescription of drug therapy for diseases of the esophagus, stomach, duodenum | 1 | 1 |
| A25.16.002 | Prescription of dietary therapy for diseases of the esophagus, stomach, duodenum | 1 | 1 |
| A25.16.003 | Prescription of a therapeutic and health regimen for diseases of the esophagus, stomach, duodenum | 1 | 1 |
| Pharmacotherapeutic group | ATX group* | International nonproprietary name | Prescription frequency | ODD** | EKD*** |
| Drugs for the treatment of gastrointestinal diseases | 0,8 | ||||
| Antacids | 0,3 | ||||
| Alhydrate + Magnesium Hydroxide | 1 | 40 ml | 560 ml | ||
| Prokinetics | 0,7 | ||||
| Domperidone | 1 | 30 mg | 420 mg | ||
| H2-histamine receptor blockers | 0,1 | ||||
| Ranitidine | 0,5 | 30 mg | 420 mg | ||
| Famotidine | 0,5 | 40 mg | 560 mg | ||
| Proton pump blockers | 0,7 | ||||
| Omeprazole | 0,25 | 20 mg | 280 mg | ||
| Rabeprazole | 0,25 | 20 mg | 280 mg | ||
| Antibacterial agents | 0,3 | ||||
| Amoxicillin | 0,5 | 2 g | 14 g | ||
| Clarithromycin | 0,5 | 1 g | 7 g | ||
| Antiparasitic agents | 0,3 | ||||
| Metronidazole | 1 | 1 g | 7 g | ||
* - anatomical-therapeutic-chemical classification ** - approximate daily dose *** - equivalent course dose
Complete medical reference book/Trans. from English E. Makhiyanova and I. Dreval. - M.: AST, Astrel, 2006. - 1104 p.
pda.rlsnet.ru
Chronic gastritis code according to ICD 10
Occupying three positions in class 29 in the medical classification, chronic gastritis (ICD code 10) is a very common disease, which is often detected not only in adults, but also in high school students.
Occupying three positions in the medical classification in class 29, gastritis, chronic code according to ICD 10, is a very common disease
Chronic gastritis most often occurs due to regular violation of the diet and consumption of large amounts of fatty, spicy, salty, sweet foods, as well as carbonated and alcoholic drinks. In addition, frequent stress, anxiety, and anxiety can provoke its appearance. This is why this disease is so widespread in the modern world.
In addition to neurological causes and poor nutrition, a number of changes in the gastric mucosa occur due to other diseases and the use of potent medications, including antibiotics.
Another widespread cause of gastritis is the bacterium Helicobacter pylori and other microorganisms. The causes that cause the chronic form also provoke the appearance of a disease such as erosive gastritis, the ICD code of which is K29.0.
This gastritis manifests itself in single attacks when irritating factors occur and passes relatively quickly without leaving a trace. However, erosive, or acute, gastritis can provoke the appearance of chronic gastritis if ignored.
With the 10th revision of the International Classification of Diseases (ICD 10), stomach diseases were included in class 29, where, in addition to chronic gastritis, its other varieties are indicated:
- K29.0 - acute hemorrhagic gastritis;
- K29.1 - other acute gastritis;
- K29.2 - alcoholic gastritis;
- K29.3 - chronic superficial gastritis;
- K29.4 - chronic atrophic gastritis (atrophy of the mucous membrane);
- K29.5 - chronic gastritis, unspecified (antral and fundic);
- K29.6 - other gastritis;
- K29.7 - gastritis, unspecified.
Despite all their similarities, each type of chronic gastritis has its own characteristics of the development and course of the disease, as well as methods of treating them
Despite all their similarities, each type of chronic gastritis has its own characteristics of the development and course of the disease, as well as methods of treating them. Changes in the gastric mucosa, causing various disruptions to its functioning, are one of the manifestations of the disease. Its most characteristic symptom is pain in the upper abdomen. It can be either sharp or dull, aching. Drawing painful sensations occur when the stomach is empty. Pain may appear 1-1.5 hours after eating.
In addition to pain, chronic gastritis often causes heartburn, nausea, and belching. There may be an unpleasant taste in the mouth and a feeling of fullness in the stomach. Often with illness, appetite decreases. Other discomfort in the abdomen also appears, such as a feeling of heaviness and bloating. Flatulence and intestinal dysfunction may begin.
In a state of remission, chronic gastritis does not manifest itself in any way, although its attacks may occur after the abuse of heavy foods or during strong emotional experiences. Typically, exacerbations of chronic gastritis occur in spring and autumn.
To prescribe effective treatment that will relieve the severity of the exacerbation and prevent the development of more dangerous diseases, it is necessary to establish the cause of chronic gastritis and its type according to the international classification.
In a state of remission, chronic gastritis does not manifest itself in any way, although its attacks can be disturbing after the abuse of heavy foods
Diagnosis is carried out precisely on the days of its exacerbation, since in a state of remission some tests will not show any changes in the body.
Blood and urine tests can look for signs of inflammation and anemia. A stool analysis will show how properly food is digested and whether there is hidden blood in the digestive tract. However, the main diagnostic procedure is FGDS - fibrogastroduodenoscopy, in which an endoscope is inserted into the patient's esophagus through the esophagus. Thanks to FGDS, it is possible to examine the diseased organ from the inside, assess the extent of inflammation of the mucous membrane, take samples of gastric fluid and a biopsy of the stomach walls.
Samples taken from the stomach are checked for the presence of microorganisms, in particular, to identify Helicobacter pylori, which causes inflammatory processes in most cases of chronic gastritis. In addition to identifying microorganisms, samples obtained during FGDS make it possible to determine the level of gastric acidity, which is extremely important when prescribing treatment.
Symptoms of the development of acute gastritis
Symptoms of stomach inflammation depend on the type of disease. The first sign of the erosive type is nausea, stomach pain and internal bleeding. There are cases when other signs are absent, and only bleeding is detected. In this case, the disease is classified as acute hemorrhagic gastritis code according to ICD 10 - K 29.0.
The catarrhal type of the disease usually develops against the background of emotional stress, poor diet, overeating or prolonged fasting. This is the simplest form of inflammation of the stomach, otherwise called acute alimentary gastritis and has an ICD code of 10 K 29.1. Treatment is carried out with medications, and traditional medicine can also be used.
The ulcerative appearance is directly related to functional stomach disorders, often manifests itself with bleeding, and can provoke the development of a perforated gastric ulcer. The cause may be infectious bacterial diseases: diphtheria, pneumonia, hepatitis, typhus.
The antral type of inflammation differs from other forms by the increased acidity of gastric secretions. The cause may be a bacterial infection, the main symptom being heartburn. It is with antral gastritis that gastric reflux can develop with the reflux of gastric secretions into the esophagus.
An attack of the acute form of the disease is not difficult to determine; the symptoms are pronounced:
- flatulence with stool disturbance;
- sour heartburn and belching;
- severe pain in the epigastric region;
- nausea and vomiting that does not bring relief;
- temperature can rise to 39 0 C;
- a gray coating appears on the tongue.
Typically, an attack develops 4 to 5 hours after the irritant.
ICD-10 code
K29.5 Chronic gastritis, unspecified
Pharm. gr. Substance Drugs for treatment
| Antacids | Hydrotalcite | Tisacid |
| Simaldrat | Gelusil | |
| Antacids in combinations | Algeldrate + Benzocaine + Magnesium hydroxide | Almagel A |
| Algeldrate + Magnesium hydroxide | Anacid forte | Gastracid | Almagel | |
| Calcium carbonate + Magnesium hydroxide | Gastrik | |
| Serotonin 5HT3 receptor blockers | Ondansetron | Latran |
| Vitamins and vitamin-like products | Retinol | Retinol palmitate |
| Gastroprotectors | Bismuth tripotassium dicitrate | Novobismol | Ulkavis | Escape |
| Other gastrointestinal drugs | Itopride | Itomed | Itopra |
| Other Metabolics | Levocarnitine | |
| Other metabolites in combinations | Birch mushroom extract + Cobalt chloride | Befungin |
| Proton pump inhibitors | Rabeprazole | Zulbex | Noflux | Razo | Rabelok |
| Macro- and microelements in combinations | Multivitamins + Minerals | Bio-Max |
| Enveloping laxatives | Aluminum phosphate | Alfogel |
| Sucralfate | Sukrat | |
| General tonics and adaptogens | Aloe arborescens leaves | Aloe juice |
| Cat's claw bark extract | Preparation "KK" Cat's claw | |
| Ophthalmic products | Norfloxacin | |
| Penicillins in combinations | Amoxicillin + Metronidazole | Helicocin |
| Nitroimidazole derivatives | Metronidazole | |
| Antidiarrheal microorganisms | Bifidobacterium bifidum | |
| Other non-narcotic analgesics, including non-steroidal and other anti-inflammatory drugs | Birch mushroom | Gastrofungin | Chaga |
| Calendula officinalis flowers | ||
| Appetite regulators | Calamus rhizomes | Calamus rhizomes |
| Laxatives | Magnesium hydroxide | |
| Myotropic antispasmodics | Bencyclane | Galidor |
| Sulfonamides | Co-trimoxazole [Sulfamethoxazole + Trimethoprim] | |
| Phthalylsulfathiazole | Phthalazol | Phthalazole tablets | |
| Enzymes and antienzymes | Rennet enzymes | Abomin |
| Enzymes and antienzymes in combinations | Hemicellulase + Bile components + Pancreatin | Panolez | Festal | Enzistal | Digestal |
| 3rd generation cephalosporins | Ceftibuten | Tsedex |
| M-Anticholinergics | Methocinium iodide | Metacin tablets | Metacin |
| N-cholinergics (ganglionic blockers) | Hexamethonium benzosulfonate | |
| Dimecolony iodide | ||
| Pempidine |
Atrophic gastritis
Atrophic gastritis refers to a precancerous form of the disease.
It is characterized by a decrease in glands, which causes a disruption in the secretion of gastric juice. In 90% of cases, the atrophic form appears due to Helicobacter bacteria entering the gastrointestinal tract.
The main signs of the disease are:
- nausea;
- heartburn;
- dull, prolonged pain in the stomach;
- dyspepsia;
- anemia;
- weakness;
- increased fatigue;
- stool disorder.
Pathogenesis
The distinctive features of chronic atrophic gastritis are considered to be a long course and progressive atrophic processes in the mucous membranes of the stomach. Atrophy affects the gastric glands, and dystrophic processes begin to prevail over inflammatory ones. Pathogenetic mechanisms ultimately lead to disruption of absorption, gland secretion and motility of the gastric muscles. Inflammatory and atrophic processes begin to spread to neighboring anatomical formations that have a common functional purpose with the stomach.
With gastritis, symptoms of general intoxication develop, and the nervous system is involved in the process. Weakness, fatigue, lethargy and headache develop. Absorption disorders lead to the development of iron and folate deficiency anemia.
Clinic
Clinically, the picture corresponds to gastritis with a reduced level of acidity of gastric juice.
- The stomach wall is thinner and sometimes stretched.
- The mucous membrane in the stomach shows a smoothed appearance and the number of folds decreases.
- The gastric pits are wide and deep.
- The epithelium in microsection has a flattened appearance.
- The glands of the stomach secrete a much smaller amount of secretion.
- Outside the blood vessels supplying the stomach, leukocytes infiltrate into the walls.
- Glandular cells degenerate.
This form of gastritis requires constant replacement therapy.
Content
Definition and general information [edit]
Chronic gastritis is a group of chronic diseases that are morphologically characterized by inflammatory and degenerative processes in the gastric mucosa.
Chronic gastritis is morphologically divided into superficial and atrophic. These terms were proposed in 1948 by the German surgeon R. Schindler. The main principle of this classification was the characteristics (preserved or lost) of normal glands of the gastric mucosa, the presence of dystrophic and dysregenerative changes in the cells of the surface epithelium and inflammatory infiltration of the lamina propria of the mucous membrane. With chronic inflammation, foci of hyperplasia develop (the severity ranges from small focal changes to hyperplastic gastritis).
Inflammation of the gastric mucosa is of two types: local (leukocyte infiltration) and immune (lymphoplasmacytic infiltration). Moreover, immune inflammation is a constant attribute of any chronic gastritis. The presence of signs of inflammation indicates active chronic gastritis, the absence suggests inactive chronic gastritis.
It must be emphasized that the defining signs of gastritis are considered to be morphological changes in the mucous membrane, but not clinical manifestations (they may not correspond to the localization, prevalence and severity of the pathological process). This indicates the need for mandatory histological examination of biopsy samples of the gastric mucosa to diagnose gastritis.
In 1990, the International Congress of Gastroenterologists (Australia) proposed a modern classification of chronic gastritis, known as the Sydney classification, which takes into account the characteristics of etiopathogenesis, morphological and endoscopic signs.
The International Sydney Classification of Chronic Gastritis (1990) distinguishes the following types of gastritis:
— type A (autoimmune);
— type B (Helicobacter);
- type C (reflux gastritis).
Also rare forms of gastritis:
- eosinophilic, indicating the state of gastric secretion: increased, preserved (normal) or secretory insufficiency (moderate and severe, including achlorhydria). The traditional staging of the disease is reflected by reference to exacerbation or remission of the process.
The new international classification of gastritis (Houston) was published at the end of 1996. It is a modification of the Sydney system and retains the basic principle of combining etiology, topography and histological characteristics in the diagnosis.
Synonyms: superficial, diffuse antral, chronic antral, interstitial, hypersecretory, type B.
Etiology: H. pylori; other factors.
Synonyms: type A, diffuse gastric body, associated with pernicious anemia.
• Chemical (synonyms: reactive reflux gastritis, type C).
Etiology: chemical irritants, bile, nonsteroidal anti-inflammatory drugs (NSAIDs).
• Radiation (etiology: radiation injuries)
• Lymphocytic (synonyms: variloform, associated with celiac disease).
Etiology: idiopathic, immune mechanisms, gluten, H. pylory.
• Non-infectious granulomatous (synonyms: isolated granulomatosis). Etiology: Crohn's disease, sarcoidosis, Wegener's granulomatosis, foreign bodies, idiopathic.
• Eosinophilic (synonyms: food allergy, other allergens).
• Other infectious. Etiology: bacteria (except N. pylory), viruses, pathogenic fungi.
Etiology and pathogenesis[edit]
Factors predisposing to the formation of CG:
• Presence of Helicobacter pylori (a gram-negative, non-spore-forming bacterium with a curved, S-shaped or spiral shape);
• Errors in nutrition - eating rough, unusual, spicy, hot food, food poisoning, eating low-quality food, irregular meals, eating in an excited, irritated state;
• Alcohol consumption, leading to disruption of mucus formation, blood circulation and regeneration of the gastric mucosa, causing its atrophy;
• Long-term smoking, which stimulates the secretion of hydrochloric acid, disrupts the tone of the lower esophageal sphincter, causing chronic inflammation in the gastric mucosa;
• Taking medications (sulfonamide drugs, salicylates, iodine drugs, NSAIDs, etc.);
• Stressful situations that disrupt the motility of the upper gastrointestinal tract, provoking spasms, against the background of which blood circulation in the gastric mucosa suffers, and duodenogastric reflux occurs. Bile reflux causes a burn of the gastric mucosa with aggressive bile acids and provokes the development of chronic gastritis;
• Food allergy accompanying the formation of eosinophilic gastritis.
• Various diseases of internal organs (severe elimination gastritis associated with the release of toxic substances through the gastric mucosa, for example in uremia);
• Insufficiency of blood circulation and external respiration function can provoke hypoxic gastritis, in which dystrophic changes in the mucous membrane are associated with microcirculation disorders.
The pathogenesis of hCG comes down to an imbalance between the factors of acid-peptic aggression of the gastric contents and the protective factors of the mucous membrane of the stomach and duodenum.
Clinical manifestations[edit]
The clinical picture of hCG depends on the state of the basic functions of the stomach. Abdominal pain is intense, often paroxysmal, localized mainly in the epigastric region, occurs on an empty stomach and decreases after eating. Early pain begins 20-30 minutes after eating.
Dyspeptic disorders may include decreased appetite, nausea, vomiting, heartburn, intolerance to fatty and fried foods, belching; bowel movements often occur, accompanied by constipation.
Chronic superficial gastritis: Diagnosis [edit]
A prerequisite for proper examination of patients is the determination of the presence of Helicobacter pylori (see Chronic gastric ulcer without bleeding or perforation)
The most accurate picture can be obtained by studying at least 5 biopsies: two each from the antrum, fundus and one from the angle of the stomach.
The main histological signs of superficial gastritis.
Main symptoms
Characteristic clinical manifestations are sensations of pain and discomfort, which are localized in the upper floor of the abdominal cavity. The appearance of pain is associated with a violation of diet and nutrition. Prolonged fasting or, conversely, excessive overeating can cause pain.
After eating, the feeling of pain, bloating and discomfort in the abdomen increases significantly. With focal gastritis, the pain is point-like in nature. Inflammation at the outlet of the stomach forms the clinical picture of antral inflammation. If the inflammation is diffuse, the entire lining of the stomach is affected. If soups and first courses are completely absent from a person’s menu, the patient abuses fatty and spicy foods, the disease becomes chronic and aggravation is regularly observed in the spring and autumn months, including moments when the regime and diet are violated. In addition to abdominal pain, the patient complains of heartburn, nausea, belching and stool disorders. In the absence of proper treatment and adherence to diet and nutrition, the superficial form turns into erosive gastritis.
Reasons for the development of the acute form
Content
There are many reasons for inflammation of the epithelium of the gastric mucosa:
- violation of diet and diet;
- food allergies;
- abuse of strong instant coffee, alcohol and carbonated drinks;
- consumption of products containing chemicals and dyes;
- long-term drug therapy and drug overdose;
- oncology of the digestive organs, trauma and surgery;
- infectious diseases of the digestive system;
- metabolic disorders;
- increased radioactive background.
The disease often occurs due to eating on the go or poor chewing of food.
Differential diagnosis
| Diseases | Clinical criteria | Laboratory indicators |
| Chronic cholecystitis | Pain in the right hypochondrium, pain on palpation in the area of the gallbladder projection, low-grade fever or periodic rises in temperature to febrile levels, intoxication | In the blood - leukocytosis, neutrophilia, accelerated ESR. Ultrasound reveals thickening of the gallbladder wall, mucus flakes in it, bile stagnation, perivascular reaction |
| Chronic pancreatitis | Localization of pain on the left above the navel with irradiation to the left, there may be girdling pain | Increased amylase in urine and blood, trypsin activity in feces, steatorrhea, creatorrhea. Ultrasound shows an increase in the size of the gland and a change in its echological density |
| Chronic enterocolitis | Localization of pain around the navel or throughout the abdomen, pain reduction after defecation, bloating, poor tolerance to milk, vegetables, fruits, unstable stool, passing of gas | In the coprogram - amilorrhea, steatorrhea, creatorrhoea, mucus, possible leukocytes, erythrocytes, signs of dysbiosis |
| Peptic ulcer | The pain is “mostly” late, 2-3 hours after eating. Occurs acutely, suddenly, pain on palpation is pronounced, tension of the abdominal muscles, zones of skin hyperesthesia, positive Mendel's sign are determined | On endoscopy, there is a deep defect in the mucous membrane surrounded by a hyperemic shaft; there may be multiple ulcers |
Treatment
Treatment tactics
Treatment goals:
– relieving the exacerbation of the disease;
– relief of pain and dyspeptic syndromes;
– eradication of Helicobacter pylori.
Therapy should be aimed at:
1. Reducing the excessive impact of aggressive factors by eliminating them (eradication of H. pylori) and neutralizing them directly in the lumen of the stomach and normalizing the secretory-motor activity of the stomach.
2. Improving the quality of the protective properties of the mucous membrane (M) of the stomach and duodenum by enhancing the formation of mucus, stimulating the secretion of bicarbonates in the antrum of the stomach, improving the trophism of the M, normalizing its reparative properties, etc.
3. Impact on the autonomic nervous system in order to correct the disturbed balance between its sympathetic and parasympathetic departments.
Non-drug treatment
Diet No. 1 (1a, 5) with the exclusion of dishes that cause or enhance the clinical manifestations of the disease (for example, hot seasonings, pickled and smoked foods). Small meals, 5-6 times a day.
Drug treatment
In accordance with the Maastricht consensus (2000) on methods of treating HP infection, priority is given to regimens based on proton pump inhibitors, as the most powerful of the antisecretory drugs. It is known that they are able to maintain a pH of more than 3 in the stomach for at least 18 hours a day, which ensures the reverse development of the inflammatory process of the mucous membranes of the stomach and duodenum. In addition, PPIs themselves have antibacterial activity. In terms of anti-Helicobacter activity, rabeprazole is superior to other PPIs /7/ and, unlike other PPIs, is metabolized non-enzymatically and is excreted primarily through the kidneys /8/. This metabolic pathway is less dangerous in terms of possible adverse reactions when combining PPIs with other drugs that are competitively metabolized by the cytochrome P450 system /8/.
First-line therapy is triple therapy.
Proton pump inhibitor (rabeprazole or omeprazole 20 mg, or lansoprazole 30 mg, or esomeprazole 20 mg) + clarithromycin 7.5 mg/kg (max-500 mg) + amoxicillin 20-30 mg/kg (max 1000 mg) or metronidazole 40 mg/kg(max 500 mg); All medications are taken 2 times a day for 7 days. The combination of clarithromycin with amoxicillin is preferable to clarithromycin with metronidazole, as it may help achieve a better outcome when prescribing second-line therapy.
In case of ineffectiveness of first-line drugs, unsuccessful eradication, a second course of combination therapy ( quadruple therapy ) is prescribed with the additional inclusion of colloidal bismuth subcitrate at 4 mg/kg (max 120 mg) 3 times a day for 30 minutes. before meals and the 4th time 2 hours after meals, before bed. The inclusion of this drug potentiates the anti-Helicobacter effect of other antibiotics.
Rules for the use of anti-Helicobacter therapy:
1. If the use of a treatment regimen does not lead to eradication, it should not be repeated.
2. If the regimen used did not lead to eradication, this means that the bacterium has acquired resistance to one of the components of the treatment regimen (nitroimidazole derivatives, macrolides).
3. If the use of one and then another treatment regimen does not lead to eradication, then the sensitivity of the H. pylori strain to the entire range of antibiotics used should be determined.
Prevention
Prevention of hiatal hernia involves strengthening the abdominal muscles, avoiding heavy physical activity, and eating right. Preventive gymnastics is useful. It is necessary to eliminate constipation in a timely manner and maintain correct posture.
We invite you to familiarize yourself with: Coccydynia of the coccyx, symptoms and drug treatment in women and men
In your diet, increase the number of steamed or boiled dishes. It is better to eat dietary meat. Eat fried, spicy, smoked foods to a minimum, as well as those with a high percentage of fat content.
When diagnosing gastroduodenitis or ulcers, treatment must be started immediately. Once a year you need to be examined by a gastroenterologist, since a hernia can occur and not make itself felt. It is better to give up bad habits.
Treatment of gastritis
As soon as the patient is diagnosed, the doctor prescribes a set of medications.
Antibiotics
Amoxicycline, Clamithroricin
IPP
Omez, Olpaza, Emanera, Pariet
Bismuth preparations
Ventrisol, De-nol
To reduce acidity
Maalox, Phosphalugel, Almagel
Enveloping agents
Sucralfate, Bismuth Dicitrate
Enzyme preparations
Pancreatin, Allahol, Cholenzyme
During treatment you must adhere to a strict diet. Avoid salty, spicy, fried and fatty foods. Stop drinking alcoholic beverages, minimize, or better yet, completely quit smoking.
By following all the doctor’s recommendations, the prognosis for treatment of chronic bronchitis is favorable. Relapses are kept to a minimum, and remission can last for many years.
Diet
Here are the basic principles of the diet for patients with gastritis:
- do not eat fatty, fried and smoked foods;
- It is forbidden to consume flour, sweets, spices;
- balanced use of vitamins;
- It is recommended to prepare dishes by steaming;
- meals should be frequent (about six times a day);
- portions should be small;
- dishes should be eaten warm and mushy;
- cook food with water, not broth.
Is it possible to use traditional medicine as a treatment for erosive gastritis?
Special forms of chronic gastritis
In the international classification of diseases, other forms of chronic inflammatory process in the stomach are also coded. According to the current classification, they act as syndromic conditions in other common diseases. Typically, types of gastritis are coded in other subheadings and are related in meaning to the underlying disease that caused their development.
The following nosological units are usually considered as special forms of inflammation:
- The atrophic-hyperplastic form of gastritis is called warty or polypous. The disease can be classified in other sections of ICD 10. In particular, the polypous form of inflammation is mentioned under code K 31.7 and is considered a gastric polyp. In addition to the heading denoting diseases of the digestive system and coded with the Latin “K”, the form is considered in the section of neoplasms as the diagnosis “Benign neoplasms of the stomach” and is coded D13.1. Gastritis in the stomach
- Hypertrophic or giant hypertrophic, called Ménétrier's disease. The disease manifests itself in pronounced hypertrophy of the folds of the gastric mucosa. The etiology is currently unknown. In the international classification it is coded K 29.6.
- A similar coding is manifested by the diagnosis of lymphocytic gastritis, which is typical for patients with celiac disease. It is characterized by the accumulation of a large number of lymphocytes in the thickness of the mucosa.
- The granulomatous variant is a manifestation of a number of other complex genetically determined and autoimmune diseases. For example, Crohn's disease, which is classified as K50, “Sarcoidosis of other specified and combined localizations” - D86.8, Wegener's sarcoidosis, which has code M 31.3.
- The eosinophilic variant has become a type of manifestation of the allergic process, characterized by eosinophilic infiltration of the gastric mucosa and the development of the inflammatory process. Sometimes coded as “Allergic and nutritional gastroenteritis and colitis” – K52.2.
- Radiation gastritis and gastroenteritis are encrypted in ICD 10 code K 52.0.
- Certain types accompany a number of infectious diseases – cytomegalovirus infection, secondary syphilitic infection, candidiasis, tuberculosis and are coded in the “infectious diseases” section.
In the latter case, the ICD-10 code is assigned according to the underlying disease that caused the inflammatory process in the gastric mucosa.
Position of the disease in the ICD system
Diseases in the international classification of diseases are in most cases divided into subsections according to etiology.
Thanks to this coding, it is possible to develop and use the latest types of pathology treatment.
For example, different types of gastritis require fundamentally different therapy. If the patient experiences a significant increase in secretion, then proton pump inhibitors must be used. If acidity is reduced, then the use of these drugs is unacceptable.
The first division in the ICD is in accordance with the lesion system. Gastritis belongs to the class of diseases of the digestive organs. The gastritis code in ICD 10 is presented as follows: K29. However, this section has 9 more subparagraphs, each of which is a separate nosological unit.
That is, K29 indicates that the patient has gastritis or duodenitis, but this is not enough to make a correct, complete diagnosis. The doctor finds out the etiology and understands the pathogenesis of the disease as much as possible, after which the final coding is carried out.
Options for the location of gastric inflammation in the ICD system:
- K29.0 - is an acute inflammatory process with the obligatory presence of bleeding (in its absence, code K25 is set, that is, ordinary erosion);
- K29.1 - this is how any acute gastritis is coded, except for the above;
- K29.2 – inflammation of the stomach caused by alcohol consumption is isolated separately;
- K29.3 - in ICD 10, erosive gastritis or superficial chronic gastritis is coded as follows;
- K29.4 – this is how chronic inflammation of an atrophic nature is written;
- K29.5 - represents a whole group of chronic nosologies, when it is not possible to clarify the etiology or type;
- K29.6 – this includes a giant hypertrophic inflammatory process or a granulomatous lesion;
- K29.7 - simply unspecified inflammation of the gastric membranes;
- K29.8 – inflammation of the mucous membrane of the duodenum or duodenitis;
- K29.9 – combined pathology in the form of gastroduodenitis.
In addition to the listed nosological units in the International Classification of Diseases, 10th revision, there are two exceptions that are in the same class, but in different sections.
These include: eosinophilic gastroenteritis and Zollinger-Ellison disease. This disease belongs to the pathologies of the pancreas and is an oncological process.